Calcaneofibular Ligament Injury
Introduction:
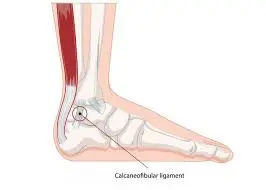
The Calcaneofibular Ligament (CFL) is one of the key lateral ligaments of the ankle, connecting the fibula to the calcaneus (heel bone). It provides stability to the ankle, particularly during inversion movements.
Injury to the CFL typically occurs due to ankle sprains, especially when the foot rolls inward excessively. Such injuries can cause pain, swelling, instability, and difficulty bearing weight on the affected ankle.
Causes of Calcaneofibular Ligament Injury:
Excessive ankle rolling or inversion, particularly while the foot is plantarflexed, is a typical cause of calcaneofibular ligament injury. This is frequently observed in high-impact sports or activities like basketball, football, or jogging that call for abrupt pauses, turns, or changes in direction.
A history of prior ankle sprains, which can result in ligament laxity and heightened susceptibility to injury, inappropriate footwear, poor neuromuscular control, and walking or running on uneven surfaces are other contributing factors.
Symptoms of Calcaneofibular Ligament Injury:
Depending on how severe the traumatic experience was, these symptoms may change. People who have partial calcaneofibular ligament tears might not have as severe symptoms as people whose calcaneofibular ligaments are entirely injured.
- Weight-bearing exercises that worsen pain
- Bruising where the injury occurred.
Differential Diagnosis:
Since the ATFL is frequently involved in CFL injuries, isolated ATFL should be taken into consideration on the differential. Crucially, ankle fractures, Achilles rupture, tendon dislocation, osteochondral damage, and fibularis tendon injury are further differentials to take into account.
- Anterior talofibular ligament injury
- Peroneal tendon dislocation/retinaculum injury
- Ankle fractures
- Osteochondral injury
- Midtarsal sprain.
Diagnosisy:
A complete physical exam is conducted after the patient’s medical history has been obtained. A range of physical exam techniques are used to assess each ankle ligament’s integrity. Another method for verifying a calcaneofibular ligament tear is magnetic resonance imaging (MRI). It is also possible to determine the extent of damage to these soft tissue structures using these sophisticated imaging examinations.
- Ultrasound: Anechoic defects or ligament stumps shifted superficially to the typically underlying peroneal tendons, may be visible in complete tears.
- MRI: A calcaneofibular ligament injury typically manifests as a thickening in the event of a sprain or chronic injury, anomalies in the ligament’s shape, partial discontinuity, and changes in signal intensity in the event of a partial tear, as well as total discontinuity and fiber retraction in the event of a complete rupture 3-5.
Along with the ligamentous changes, there may be indications of tenosynovitis of the peroneal tendons or changes in bone marrow signals at the calcaneal and distal fibular insertion sites.
History and Physical Examination:
Patients may report pain, redness, swelling, cracking sounds, and stopping their activity. As a result, the physical examination should include palpation, inspection, and specific techniques such as the talar tilt test and anterior drawer test.
Similar to this, the talar tilt test can be carried out with the patient’s foot in a neutral posture while the examiner tilts the ankle inward. There is a 90% risk of lateral ligament rupture if physical examination results show ecchymosis and localized pain 4–5 days after the injury.
There is a 72% chance of ligament damage in those who have pain when the CFL is palpated. With a sensitivity of 96.4% to 99.6%, this evaluation method is useful for ruling out ankle fractures.
Evaluation:
Individuals who test positive on the Ottawa ankle test ought to be referred for an ankle X-ray. It is noteworthy that less than 15% of cases involve ankle fractures. Dynamic imaging is a benefit of ultrasound, and MRI can be used when there is a strong suspicion of ligament damage.
The clinician’s skill and level of experience determine how accurate the ultrasound is. When it comes to identifying ligamentous damage, its sensitivity and specificity are 92% and 64%, respectively. The excellent sensitivity (93% to 96%) and specificity (100%) of MRI allow clinicians to use it when there is a high clinical suspicion of fracture.
Treatment of Calcaneofibular Ligament Injury:
When treating CFL injuries, conservative management is frequently successful. Because of this, every biological stage presents a different window for therapeutic intervention.
A brace or tape can then be used to allow for a return to activities. Since functional stress encourages remodeling, immobilization during the proliferative period is discouraged. Oral medications like NSAIDs are available over-the-counter to help alleviate pain.
The results for both patients were ideal. Although the overall clinical outcome of conservative versus surgical intervention is comparable, surgical intervention must be evaluated on an individual basis.
Surgical Treatment:
Patients who have persistent ankle joint instability following conservative treatment or who have had a total rupture of the calcaneofibular ligament may require surgery. To repair the calcaneofibular ligament tear, surgery can be required.
The ligament’s remaining healthy tissue is sutured back together or reattached to the bone after the damaged sections have been cleansed. The type of tear determines the precise incision and method.
Prevention of Calcaneofibular Ligament Injury:
Regular strengthening and balancing exercises are essential for keeping strong and stable ankles and preventing calcaneofibular ligament injuries. Ankle sprain risk is decreased and coordination is enhanced by proprioception training, such as that done with a balance board.
Additional protection can be obtained by wearing supportive, well-fitting shoes and applying ankle braces or taping when participating in sports or other high-impact activities. Stretching and a decent warm-up are also essential before beginning any physical exercise.
To further reduce the danger of calcaneofibular ligament injury, avoid slick or uneven surfaces and gradually increase the intensity of your workouts.
Prognosis:
Given that 25% of patients are anticipated to miss work or school, it is crucial to have a conversation about returning to play or work at the time of diagnosis. In addition, patients might endure chronic pain or instability. Furthermore, symptoms have been recorded by 32% of patients for up to 7 years following the initial damage.
Due to bias in individual studies, Thompson et al.’s systematic review revealed that traits like range of motion, weight-bearing status, and pain severity were inconsistent predictive factors. These clinical results can, however, be used cautiously to help patients recover as expected.
Complications of Calcaneofibular Ligament Injury:
Although they are not sentinel events, lateral ankle injuries can have long-term effects. Low-grade ankle sprains frequently result in lateral compartment reinjury. Patients may have pain and instability, which limits their ability to move around functionally.
Conclusion:
An injury to the calcaneofibular ligament, which is frequently linked to lateral ankle sprains, can cause discomfort, edema, instability, and trouble bearing weight. For the best recovery, early diagnosis and suitable treatment such as rest, immobilization, physical therapy, and in certain situations, surgery are crucial.
Most people can resume their regular activities and avoid recurring ankle injuries with prompt rehabilitation that focuses on regaining strength, stability, and proprioception.
FAQs
How is a calcaneofibular ligament diagnosed?
The extent of injury to these soft tissue structures can also be determined by these sophisticated imaging tests.
How do you tell if your calcaneofibular ligament is torn?
The following symptoms and/or indicators may be present in the injury history: The lateral side of the ankle joint is where the majority of the pain is felt. Edema is present and gets worse the more severely a sprain occurs. Ecchymosis is present; its severity rises with a sprain.
What is a calcaneofibular ligament Grade 2 injury?
Moderate Grade 2 Sprain
Ankle pain and edema are moderate, and recovery usually takes two to three weeks.
In what way is a calcaneofibular ligament taped?
The anterior talofibular ligament and calcaneofibular ligament will be stabilized as a result.
Is surgery necessary for a CFL tear?
Although most of these injuries can be successfully treated non-surgically, certain patients may develop chronic instability that necessitates surgery.
How may a calcaneofibular ligament tear be detected?
Talar Tilt Test: Although the primary purpose of this test is to assess the calcaneofibular ligament’s (CFL) integrity, it can also provide important insights into the ATFL.
References
- Le, M. Q. T., & Tiu, T. K. (2023, August 8). Calcaneofibular ligament injury. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557378/
- Drhaytmanek. (2024, August 14). Calcaneofibular ligament (CFL) tear. Sport Foot & Ankle. https://sportsfootankle.com/calcaneofibular-ligament-cfl-tear-foot-ankle-specialist-vail-co/
- Feger, J. (2020). Calcaneofibular ligament injury. Radiopaedia.org. https://doi.org/10.53347/rid-80332
- The role of calcaneofibular ligament (CFL) injury in ankle instability: Implications for surgical management. (n.d.). https://www.isakos.com/GlobalLink/Abstract/1803