Ulnar Collateral Ligament Injury
Introduction:
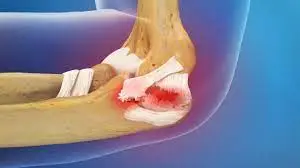
The ulnar collateral ligament (UCL) is a key stabilizing ligament on the inner side of the elbow, connecting the humerus to the ulna. UCL injuries often occur due to repetitive stress from overhead motions, commonly seen in athletes like baseball pitchers and javelin throwers.
An internal elbow injury is caused by damage to the ulnar collateral ligament (UCL). Most unusually, it is referred to as a baseball player’s injury and is most commonly an overuse injury.
The ulnar collateral ligament (UCL), which connects the ulna (one of the forearm bones) to the humerus (upper arm bone), is a crucial stabilizing ligament found on the inside of the elbow. Usually caused by sudden trauma or repetitive stress, a UCL injury happens when this ligament is overstretched, partially torn, or ruptured.
Due to the considerable valgus force put on the elbow, this injury is frequent among athletes, particularly baseball players and athletes who throw objects above. instability, reduced throwing velocity, and edema are possible symptoms. Recovery and complete function restoration depend on a proper diagnosis and course of treatment, which might include anything from rest and physical therapy to surgery.
What is the ulnar collateral ligament (UCL)?
On the inside of the elbow lies a robust band of tissue called the ulnar collateral ligament (UCL). When throwing or making overhead arm motions, it maintains the elbow joint’s stability.
The UCL may become irritated and inflamed, stretch, tear partially, or tear entirely as a result of repetitive overhead motions or a fall on the outstretched arm. Loss of function, pain, and elbow joint looseness are common symptoms of ligament injury.
The most common ligament damaged by repeated overhand throwing is the UCL. It is commonly referred to as the ligament that baseball pitchers sustain the most injuries to.
Work of the ulnar collateral ligament:
- Three bones meet at the elbow joint: the humerus, the upper arm bone, and the ulna and radius, the lower arm bones.
- The joint is a combination of a pivot joint and a hinge. The pivot enables the lower arm to twist and rotate, while the hinge permits the arm to flex and extend.
- The little finger side of the elbow is where the UCL is situated. It is composed of three tissue bands that join the ulna and humerus. Three bands are present: the diagonal (transverse), the back (posterior), and the front (anterior). The most important band for maintaining elbow stability is the anterior band.
Epidemiology:
Athletes who participate in overhead-throwing sports like baseball, softball, and javelin throwing frequently sustain ulnar collateral ligament (UCL) injuries. Because of the great pressures placed on their elbow joints, these injuries are more common in pitchers and frequently affect younger people.
There are more males than females in the majority. From amateur to professional athletes, UCL injuries can happen at any level of competition. These injuries are usually caused by the repetitive strain and stress that these activities put on the ligament.
Males are more likely than females to sustain ulnar collateral ligament injuries, with a 60% prevalence in the former group. Certain sports, such as baseball, javelin, and skiing, are among the specific patient populations that may be at risk. Moreover, this injury pattern may be caused by straightforward mechanisms like falls in elderly or disabled people.
Classification of ulnar collateral ligament injury:
UCL sprain injuries come in three different grades:
- Grade 1: Although the ligament is stretched, it is not injured.
- Grade 2: The ligament may be partially torn and is expanded.
- Grade 3: There is total ligament rupture.
Causes of ulnar collateral ligament (UCL) injury:
When throwing, the UCL prevents the elbow from being abducted. Injury may result from severe or recurrent episodes of valgus stress on the UCL. Due to their comparable throwing motions, baseball pitchers and javelin throwers frequently sustain UCL damage. Doctors think UCL injuries are caused by repetitive motions, particularly when pitching in baseball. Additionally, according to medical professionals, adolescents who throw more than 85 times in a year or when they are weary are at a much higher risk of suffering a UCL injury.
Players in water polo, ice hockey, racquet sports, and gridiron football have also received treatment for UCL injuries. The risk of a UCL injury is increased by certain overhead motions, such as those made when pitching in baseball, serving in tennis, or spiking in volleyball. The elbow is flexed, the shoulder is externally rotated, and the shoulder is horizontally abducted during the cocking phase of pitching. The UCL is slightly stressed in this position, but as the shoulder is further externally rotated during a throw, the stress increases. The UCL is stretched more while under stress, which results in strain.
Arm cocking and acceleration during the overhead throwing motion cause valgus stress on the medial elbow. At the end of the arm-cocking phase, valgus tension begins to develop. The elbow flexes from 90° to about 125°, the forearm is in nearly complete supination, and the shoulder rotates vigorously internally during the transitional phase from arm cocking to arm acceleration. When the elbow is released from late cocking, it quickly stretches from about 125° to 25°. The UCL experiences severe tensile strain and valgus stress as a result.
Poor throwing technique, excessive use, high throwing velocity, and throwing certain pitches, such as curveballs, can all lead to UCL injuries. Irritation, microtears, or ruptures of the UCL can result from poor mechanics and excessive repetition of these overhead movements. UCL injuries, capsular stiffness in glenohumeral internal rotation deficit (GIRD), and scapular dyskinesis can all be linked to kinetic chain dysfunction caused by inadequate lower extremity strength, core strength, and stability. Baseball players rarely sustain UCL injuries as a result of isolated, stressful incidents. Instead, minor chronic strains and tears that build up over time are more likely to cause them.
Overuse, wear, and tear injuries:
- Overuse is the cause of UCL injury in far too many cases. Overhand throwing is an example of a repetitive motion that puts stress on the ligament. The UCL stretches, becomes inflamed, and the tissue degrades from tiny microtears after months or even years of continuous, intense use.
- The elbow joint becomes “unstable” or loose. One end of the ligament may pull away from the bone, the UCL may tear partially or entirely, or it may become strained and inflamed.
Traumatic injuries:
- A blow or impact to the elbow causes traumatic damage to the UCL.
- They’re not injuries from overuse.
- One example is a fall that lands on the outstretched arm “to break the fall.”
- This could cause a fracture or dislocation of the elbow, which could harm the UCL.
Symptoms of ulnar collateral ligament injury:
Mild to moderate symptoms involve:
- Inner elbow pain and soreness occur during or after an activity involving the above arms.
- pain when the arm moves quickly.
- unsteady or weak elbow sensation.
- A hand grip that is awkward or weak.
- reduction in throwing force or speed.
Symptoms of a torn ligament Involve:
- noticing an abrupt pop in the elbow’s inner elbow.
- severe pain.
- loss in throwing ability.
- Numbness and tingling in the ring and tiny fingers. This indicates that there is additional pinching or damage to the ulnar nerve.
Diagnosis:
In addition to reviewing the patient’s medical and athletic history, the doctor typically an orthopedic or sports medicine specialist will do a physical examination. He will assess range of motion, elbow strength, elbow stability, arm muscle mass, and appearance during the examination. He will also be able to look at the shoulder. Additionally, they will inquire about the patient’s pain location.
Your provider may request the following tests:
- The Valgus stress test is a physical examination in which the doctor raises the lower arm 30 degrees before placing their fingers on the UCL. Then they draw the lower arm outside and slowly press the elbow inward toward the body. Pain and a feeling of looseness at the elbow joint indicate a favorable examination.
- Imaging tests such as computed tomography (CT) and X-ray show images of the bones, stress fractures, and other bone problems that may be causing elbow pain and restricted range of motion. Unlike the UCL, they do not display soft tissue directly.
- A magnetic resonance imaging (MRI) scan can reveal damage to soft tissues such as ligaments and tendons. Additionally, it could reveal tiny fractures that X-rays miss.
- An arthrogram is an MRI combined with an injection of dye into the elbow joint to help visualize difficult-to-detect issues.
Treatment of ulnar collateral ligament injury:
The degree of the ulnar collateral ligament (UCL) injury and the degree to which the patient wishes to use the arm for demanding overhead motions or throwing activities determine the course of treatment. The healing process of a mild UCL tear can occur naturally. Nonsurgical treatments can help a person feel less pain and discomfort.
Medical Treatment:
- Rest.
- NSAIDs, such as naproxen and ibuprofen. If you require a prescription-strength NSAID, ask the clinician about it.
- Ice: To reduce pain and swelling, apply ice to the elbow once a day.
- Physical therapy: To strengthen the muscles surrounding the elbow, begin physical therapy.
- Platelet-rich plasma (PRP) injections: A small volume of the patient’s blood is extracted, and the platelets are isolated from other blood components. The injured area receives an injection of platelets. PRP injections may be beneficial for people who have a partial UCL tear.
Partial tears may be treated with splinting or immobilization, but it is still wise to have a hand surgeon evaluate the patient. Three weeks is the usually suggested immobilization period. Physical therapy and rehabilitation can then be applied to these nonsurgically treated conditions. In addition to strengthening exercises, therapy involves both passive and active methods. When the patient is not actively receiving physical treatment, immobilization is advised for an extra three weeks, for a total of roughly six weeks of immobilization therapy. After this period, patients who continue to have pain or weakness should be referred for surgery.
According to the majority of published research, patients who have surgery after suffering total ulnar collateral ligament tears recover effectively and experience few serious aftereffects. According to one study on sports-related injuries, there was a 10.3% postoperative complication rate and an overall 98.1% successful return to play following surgery without a discernible decline in performance. For full tears, early surgical intervention is typically necessary to avoid the formation of the Stener lesion, as a consequence. This issue arises when the injured end of the ulnar collateral ligament migrates superficially and rests on top of the muscle and aponeurosis of the adductor pollicis. Surgery is advised as the final course of treatment since the ligament cannot recover properly due to this changed structure.
Physical Therapy Treatment:
When it comes to treating and recovering from ulnar collateral ligament (UCL) injuries, physical therapy is crucial. Physical therapy aims to strengthen the surrounding muscles, increase the range of motion, lessen pain, and eventually get the athlete back to their sport.
Pain Management:
To control pain and inflammation, modalities including ultrasound, heat, and ice may be applied.
Certainly, the following fundamental range-of-motion exercises can be included in the rehabilitation process for an ulnar collateral ligament injury: mild exercises to maintain and enhance elbow range of motion:
Elbow Flexion and Extension:

- Flex the elbow slowly to the extent that it feels comfortable, then fully extend it. Try to gradually increase the range of motion without producing pain by repeating this action a few times.
Pronation and Supination:
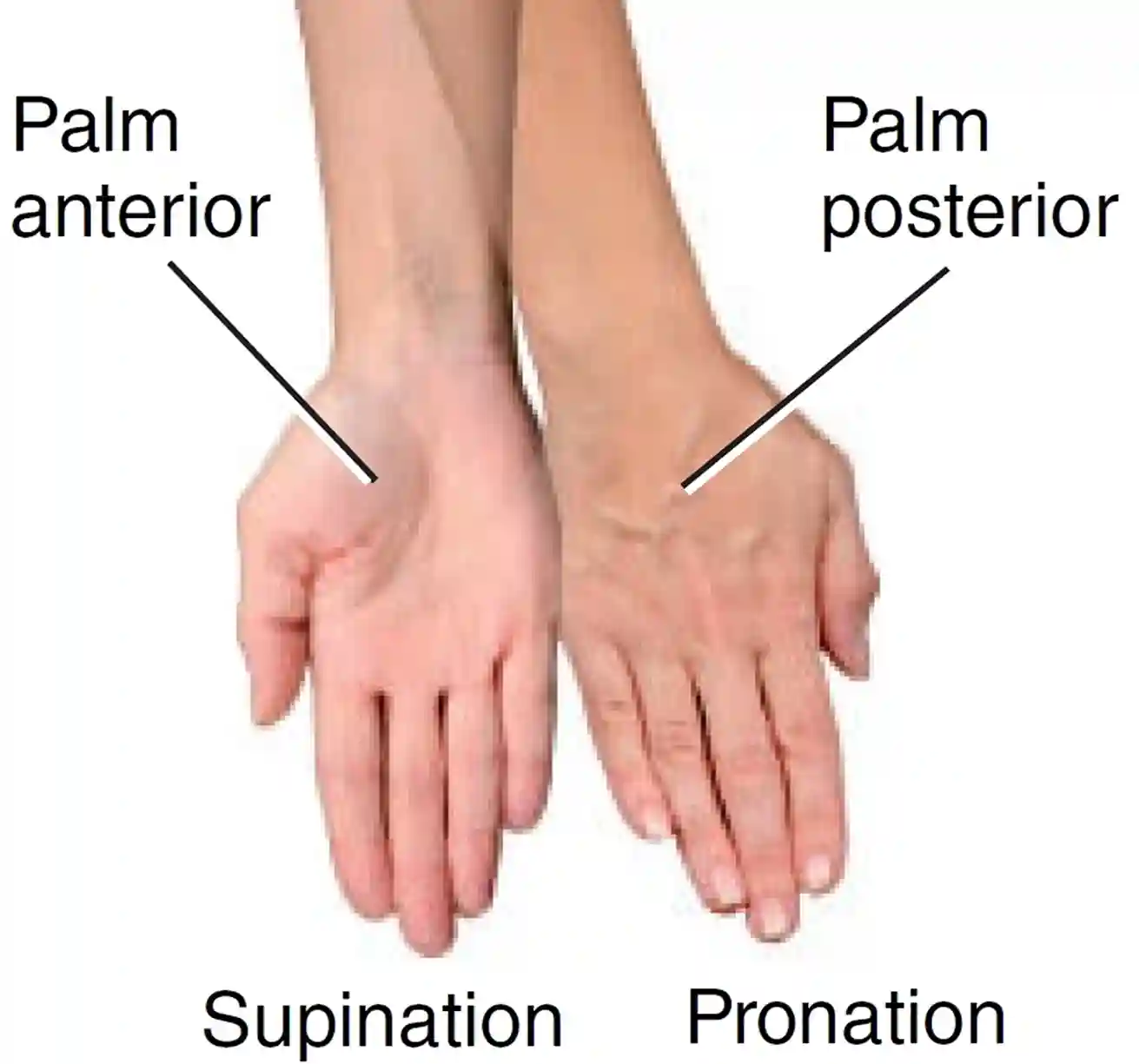
- Gently and easily rotate the hand palm up (supination) and then palm down (pronation) while seated with the forearm supported on a table.
Wrist Flexor Stretch:
- Use the other hand to assist in stretching the wrist flexor muscles as you slowly flex the wrist, bringing the fingers toward the inner forearm. Hold the position for 10 to 20 seconds and repeat a few times.
Finger Walking:
- Place the hand palm up on the table and “walk” it up and down the table surface with the fingers while maintaining a stable elbow.
Active Assisted Flexion:
- Use the opposite hand to help gradually flex the damaged elbow, assisting in obtaining a somewhat larger range of motion than a person may manage on their own.
Towel Assisted Stretch;
- It is always best to work with a professional to create a customized exercise plan that meets your specific needs. To help stretch the wrist and elbow flexors, hold a small towel in your hand and slowly pull the towel with your other hand. Keep in mind that these exercises should be performed in a pain-free range and should not cause any pain. If you experience any pain or unusual sensations during these exercises, stop right away and consult your physical therapist or healthcare provider.
Strengthening exercises:
Targeted exercises to strengthen the shoulder, wrist, and forearm muscles to improve support for the injured UCL. Undoubtedly, the following strengthening exercises can aid in the recovery from an ulnar collateral ligament injury: Always start with low resistance and work your way up, keeping in mind pain and discomfort.
Wrist Flexor Curls:
- Perform two to three sets of ten to fifteen repetitions and hold a light dumbbell or resistance band palm up. Slowly curl your wrist joint upward and then lower it.
Wrist Extensor Lifts:
- Hold a resistance or weight in your hand with the palm facing down. Raise the wrist, then bring it back down. Perform a set of one to three reps.
Wrist Pronation and Supination:

- Have a resistance band or a light dumbbell on your hand. To go from palm up to palm down and back again, rotate your wrist. Perform a set of one to three reps.
Wrist Radial and Ulnar Deviation:
- Hold a resistance band or weight in your hand. Rotate the wrist first in the direction of the elbow (radial deviation) and then in the direction of the little finger (ulnar deviation). Perform a set of one to three reps.
Shoulder External Rotation:
- Attach a resistance band at waist height to a sturdy platform, keep the band in place, and rotate the forearm out from the body to engage the shoulder’s external rotator muscles. Perform 1-3 sets of 10–15 repetitions.
Shoulder Internal Rotation:
- Rotate the forearm in the direction of the body, just like you would with the external rotation. Perform 2-3 sets of 10–15 repetitions.
- Don’t forget to employ controlled motions, keep your form correct, and stay away from any painful or uncomfortable actions. Additionally, it is advised to speak with a physical therapist or other healthcare provider before beginning a new fitness program, particularly during the recovery phase. Depending on particular needs and circumstances, they might offer tailored advice.
Surgical Treatment:
- UCL direct repair. It may be possible to repair the UCL ligament if it was pulled off the bone by a single traumatic event.
- Rebuilding the UCL (Tommy John Surgery). The doctor will recommend UCL reconstruction if a patient has an unstable or torn UCL and nonsurgical treatments are ineffective in relieving pain, or if the patient is an athlete and wishes to continue throwing or performing other demanding overhead arm motions.
- In this procedure, the surgeon removes a tendon from a donor or another part of the body. The tendon serves as the replacement UCL and is attached to the ulna and humerus. To reinforce the new graft, the residual portions of the original UCL might be affixed.
- Regaining elbow stability and range of motion, strengthening the elbow, and reducing pain are the objectives of surgery.
Why does Tommy John Surgery refer to UCL reconstruction?
The procedure is named for the first person to have it done. Tommy John tore his UCL ligament in 1974 while playing baseball in the major leagues. He sat out a season but is the 1st pitcher to have the surgery and successfully get back to baseball.
Complications of UCL reconstruction surgery?
Some consequences, like the risk of infection or anesthesia-related problems, are the same as those that people have after any surgery. Additional issues unique to UCL reconstruction include:
- The new graft may stretch or burst. In this situation, a second surgery with a fresh graft may be performed.
- Ulnar nerve irritation: The elbow joint is surrounded by the ulnar nerve.
- To avoid more aggravation, the surgeon may need to reposition it in front of the elbow joint.
Prognosis:
Despite the lengthy period of immobilization, partial tear of the ulnar collateral ligament typically heal successfully when treated with splinting alone. A small percentage of patients may experience ongoing pain and stiffness. In the case of full ulnar collateral ligament tear, surgery can usually be carried out without any difficulties, as was covered in the treatment and management section above.
Chronic alterations in the metacarpophalangeal joint space can be seen in those who get Stener lesions or who don’t receive treatment. In general, the patient should refrain from working or participating in sports for at least six weeks.
Complications:
Partial tears and strains can usually be treated conservatively with rest, ice, elevation, splinting, and pain management using over-the-counter anti-inflammatory and analgesic medications. Loss of function may arise from an early return to activities without proper rehabilitation. Anesthesia, the danger of infection after surgery, and possible nerve damage are all intrinsic risks of surgery. Loss of function could also occur if more serious injuries are not surgically repaired.
Prevention:
- Ulnar collateral ligament injury can be avoided with appropriate elbow movement technique, correct training, and resting when elbow pain occurs.
- Limiting the number of pitches and requiring recovery can help players avoid injuries.
- Additionally, appropriate throwing techniques (avoid sidearm throwing), stretching, weight training, and conditioning can all help lower the risk of UCL injury.
Conclusion:
An injury to the ulnar collateral ligament is an injury to the inner elbow. Known most commonly as a baseball pitcher’s arm injury, it is mostly an overuse injury. However, anyone who frequently performs demanding overhead arm motions may sustain this injury.
Elbow pain and soreness are among the symptoms. Some people may experience an unexpected pop in the inner elbow. Simple remedies like rest, ice, medicine, and physical therapy may help your elbow heal if you’re not an athlete or use repetitive overhead arm motions.
A tendon from another part of the body or a donor is used as a substitute ligament in Tommy John surgery. Depending on the extent of your injury and the amount of time you need to perform demanding overhead arm motions, you and your healthcare physician will choose the best course of action.
FAQs
When your UCL is injured, should you wear a brace?
The Advice of Bracing Experts
usually an immobilizer if the injury is severe enough, and a hinged brace to protect the ligament. Using a brace to treat the injury would be comparable to using one to treat a knee ligament injury.
What severity is a UCL injury?
The ligament that runs on the inside of the elbow to support it during specific activities, including throwing, is called the ulnar collateral ligament (UCL). The elbow may become unstable, cause pain, and impair function if this ligament is teared or injured.
Can someone with a UCL tear straighten their arm?
Additional symptoms include: If there is an acute tear, swelling and bruising at the injury site in the inner elbow and upper forearm (after 24 hours). losing control of the ball or being unable to throw at full speed. stiffness or difficulty in extending the elbow.
Is it possible to massage your UCL?
Elbow UCL sprains can be effectively treated with rest, physical therapy, chiropractic adjustments, massage, and in extreme situations, Tommy John surgery. It’s critical to collaborate with your physician or physical therapist to identify the most effective treatment plan for your unique requirements.
How much time does it take for UCLs to heal?
Not requiring surgery:
If you have a UCL tear, recovery may take a few weeks to many months. How much range of motion you want to regain will determine how long your recovery takes.
Which muscles provide UCL protection?
These muscles consist of the Palmaris Longus, Pronator Teres, Flexor Digitorum Superfiscialis, Flexor Carpi Ulnaris, and Flexor Carpi Radialis. These do an excellent works of absorbing the valgus load and safeguarding the UCL with that particular attachment to the medial epicondyle and their corresponding distal attachments.
Can someone with a torn UCL lift weights?
What signs of a UCL tear are present? The inside of your elbow may hurt, especially when you’re pitching. You should still be able to carry out your everyday tasks, including working out and lifting weights.
Can a tear in the UCL heal itself?
The ulnar collateral ligament may mend itself if the damage is small. For the ligament tear, non-surgical treatment comprises rest, ice, and medicines to reduce swelling and pain. Additionally, rehabilitation would be an essential component.
How is the ulnar collateral ligament treated?
Nonsteroidal anti-inflammatory drugs, including naproxen, ibuprofen, and aspirin. Ice should be applied to the elbow every day until the pain and swelling subside. You can start physical therapy to strengthen the muscles surrounding your elbow to make up for the damaged ligament once the pain has subsided.
Which workouts are beneficial for pain in the UCL?
Stretching can aid in the healing of injured muscles and the restoration of joint mobility. The forearm stretch, wrist radial and ulnar deviation, and wrist extension and flexion are some of the best stretches for UCL sprains. Without overstretching the sprain, it aids in maintaining the length and flexibility of the muscles.
How may damage to the ulnar collateral ligament be repaired?
How can a UCL tear be treated? The severity of the injury determines the course of treatment for a torn UCL. Minor injuries can frequently be healed with rest and physical treatment. More serious injuries could require surgery, especially for pitchers and other athletes.
Are elbow ligaments self-healing?
When injured, elbow ligaments typically recover without surgery. In actuality, it is quite uncommon for elbow injuries to result in lifelong instability. Elbow stiffness is far more common, though. An elbow dislocation is the most severe injury to the elbow ligaments.
What is the treatment of ligament injuries using Ayurvedic medicine?
Panchakarma, physical therapy, prescription drugs, exercise, dietary guidance, and lifestyle modifications are among the treatments. Panchakarma: based on where the damage occurred, either Nasya, Virechana, or Basti. Outside: Dhara, Pichu, Lepa, Upanaha, Kashaya Seka Sthanika Basti, PPS, SSPS, and Abhyanga.
How should torn ligaments be treated?
Ibuprofen and naproxen are examples of nonsteroidal anti-inflammatory medications that can lessen the pain and inflammation caused by an ACL tear. Prescription medication use for a brief period of time could potentially be an alternative.
How can my ligaments heal more quickly?
For a knee injury, early care may involve:
Rest. To lessen the swelling that develops within hours of an accident, apply an ice pack. Compression (of a brace or elastic bandage) height painkillers.
References:
- Thakkar, D. (2023, August 31). Ulanar Collateral ligament injury – Cause, symptoms, treatment. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/ulanar-collateral-ligament-injury/
- Wikipedia contributors. (2024c, September 17). Ulnar collateral ligament injury of the elbow. Wikipedia. https://en.wikipedia.org/wiki/Ulnar_collateral_ligament_injury_of_the_elbow
- Ulnar Collateral Ligament (UCL) injuries. (2025, March 19). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22760-ulnar-collateral-ligament-ucl-injuries