Rectus Femoris Muscle
Anatomy of Rectus Femoris Muscle
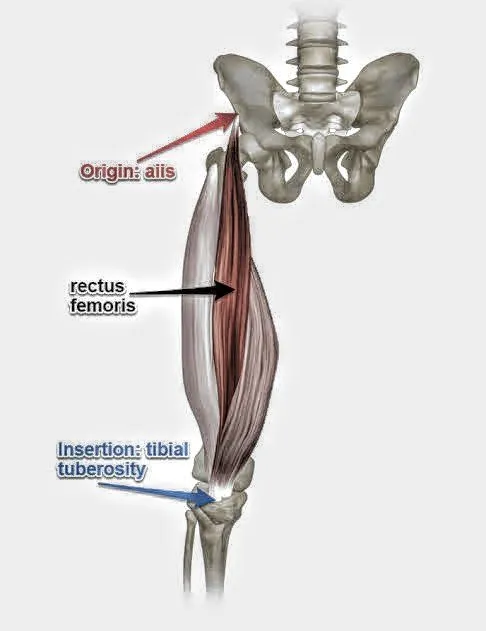
The rectus femoris muscle is one of the four quadriceps situated in the front of the thigh. It is unique among the quadriceps as it crosses both the hip and knee joints, making it a biarticular muscle.
This muscle causes two actions, it allows the hip to flex and the knee to extend. This dual-joint action makes it crucial for a wide range of movements, from walking and running to kicking and climbing stairs.
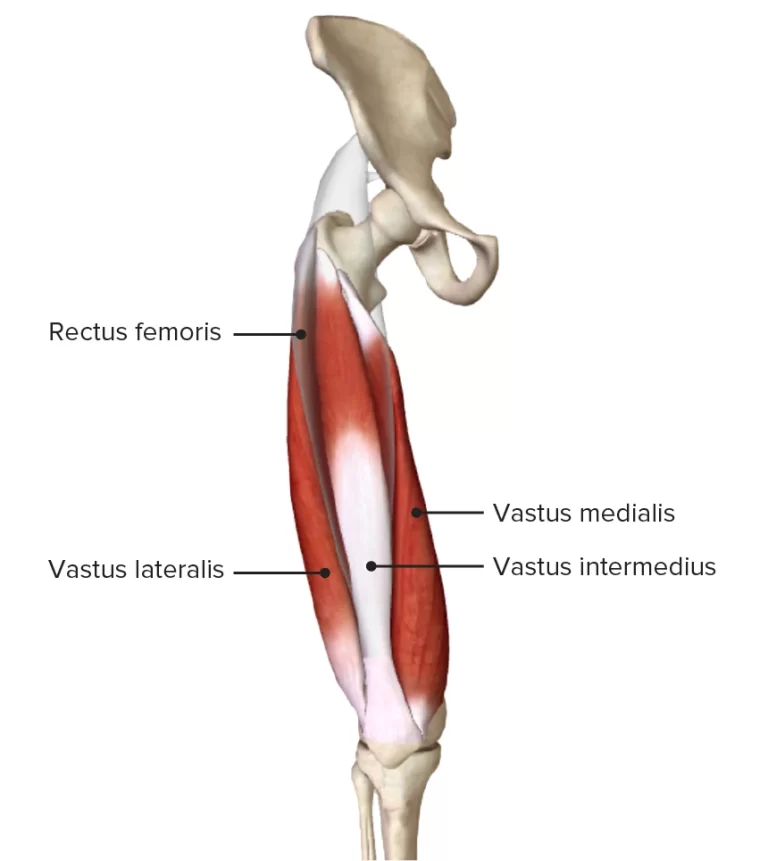
The vastus intermedius exhibits a superior anatomical orientation, while the vastus medialis and lateralis demonstrate a superomedial positioning. With the help of the iliopsoas, It draws the thigh towards the chest while extending the leg.
Origin
Rectus femoris originates from the anterior inferior iliac spine (straight head) and the supraacetabular groove (reflected head) on the ilium. The two heads combine to form a common muscular belly that covers the anterior side of the thigh and runs down it nearly vertically.
A thick tendon that penetrates into the patella’s base is where the muscle fibers converge. The iliofemoral ligament can occasionally give rise to a third head in the rectus femoris.
Insertion
Through the quadriceps tendon, the rectus femoris inserts into the base of the patella.
Innervation
The Rectus femoris gets its nerve supply from the femoral nerve. The femoral nerve arises from L2-3-4.
Blood supply
The descending LCF artery, a vital blood vessel, nourishes the rectus femoris muscle.
Lymphatic drainage
The lymphatic fluid from the veins of the anterior thigh region flows into the superficial inguinal lymph node. These veins run downwards into the lateral aorta and external iliac lymph nodes.
Functions
Hip flexion
Hip flexion is made possible by the biomechanical connection between the rectus femoris and iliopsoas muscles during knee flexion.
The rectus femoris, or hip flexor, collaborates with the iliopsoas during the “Toe off” phase of gait training.

Knee extension
The quadriceps muscles, including the rectus femoris, aid in knee extension.
The quadriceps tendon is formed by the combined tendinous insertions of the rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius muscles.

Exercises
Stretching Exercises of Rectus Femoris
- Standing Quad Stretch
- Stand facing a wall.
- Take a single stride forward while bending your knee to a 90-degree angle.
- Lean forward, keeping your back straight, until you feel a stretch in the front of your thigh.
- After 30 seconds of holding, switch legs.

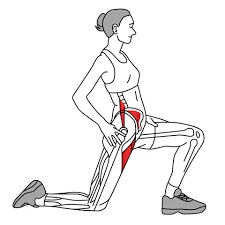
2. Kneeling Quad Stretch
- Place the other foot flat on the floor in front of you while kneeling on one knee.
- Lean back slightly, keeping your back straight.
- Pull your heel toward your buttocks by reaching back and grabbing your ankle.
- Hold for 30 seconds, then switch legs.
3. Hip Flexor Stretch
- Kneel on one knee, placing the other foot flat on the floor in front of you.
- Lean forward, keeping your back straight, pushing your hips forward.
- Hold for 30 seconds, then switch legs.

Strengthening Exercises
- Straight Leg Raises
- Perform straight leg raises by lying on your back with one leg extended upwards and the other leg bent.
- Slowly lift the extended leg towards the ceiling, then lower it back down. Repeat 10-15 times per leg.

2. Knee Extensions
- To perform seated knee extensions, Sit upright in a chair with your feet flat on the floor.
- Secure a weight or resistance band around your ankles.
- Extend your one leg straight.
- Return to the starting position by slowly lowering your leg.
- Repeat 10-15 times per leg.
3. Bulgarian Split Squat
- Stand facing away from a bench or box, about two feet away.
- Place the top of one foot on the bench, keeping your other foot flat on the floor.
- Lower your back knee towards the floor, keeping your front knee aligned with your ankle.
- Repeat with the other leg.

4. Static Lunges
- Stand with your feet hip-width apart.
- Take a single stride forward while bending both knees to a 90-degree angle.
- Push back up to the starting position.
- Repeat with the other leg.

Cool-down (5 minutes):
- Hold a quad stretch for 30 seconds on each side.
- Hold a hamstring stretch for 30 seconds on each side.
- Child’s pose for 30 seconds.
Anatomical Variantions
From the rectus femoris other accessory muscles can also originate. A muscle slip that starts in the acetabulum and inserts straight into the vastus lateralis muscle is one example of an anatomical variant. Rectus femoris can also have 2 heads, where a single tendon arises from the Anterior inferior iliac spine (AIIS), And there can be the absence of the acetabular origin.
Surgical Implications
Whenever the injury to the rectus femoris occurs, one can feel a tearing sensation and Sudden pain. In subacute injuries, the pain increases gradually and the intensity can be mild to moderate, which is exacerbated by running. For treatment and diagnosis purposes ultrasonography and MRI is used to examine the injury to the muscle.
Proximal rectus femoris rips are associated with sports, such as soccer that involve a lot of kicking and running activity. These rips are uncommon. The direct head of the muscle is associated with this injury more as compared to the indirect head, but if total avulsion takes place both of the heads will be involved.
In an acute case, where a single head of rectus femoris is torn, it is treated conservatively. It can be re-occur. If there is total avulsion or Intermittent rip of single-head can be treated surgically. Prognosis is observed good in these conditions, with this surgical procedure patients are able to become functional as before.
Distal tendon ruptures are often associated with distal rectus femoris torsen. This affects how well the quadriceps muscle works overall. Quadriceps tendon rip usually decreases functionality, which Generally necessitates a surgical procedure.
Quadriceps Tendon Ruptures
The patients, who are aged 40 years and above are more prone to distal quadriceps tendon rupture. In comparison to patellar tendon ruptures, distal quadriceps tendon ruptures are more prevalent.
Surgery is generally recommended unless the patient’s underlying health conditions outweigh the potential benefits of repair. Only partial tears that maintain the knee’s extension function can be treated without surgery.
In the post-surgical stage, the knee is immobilized with a hinged knee brace for at least 2-3 weeks or a knee immobilizer can also used. In this brace, the knee is held in extension, which depends on the degree of partial Trauma. Following multiple clinical evaluations, the patient was promptly initiated into an intensive physical therapy program to mitigate the risk of developing knee stiffness and quadriceps muscle wasting.
During locomotion, wearing of knee brace is advised to a patient, Until the patient exhibits adequate quadriceps muscle function. Assistance is provided to the knee by the brace, to bolster the knee joint’s dynamic stabilization mechanisms. Any injuries affecting the musculotendinous structures of the knee joint Should be managed according to the same rehabilitation paradigms and parameters.
Primary repair is also rehabilitated by previously explained techniques after the post-op stage. For approximately two weeks the extended knee is immobilized in a brace, post-surgery. Partial weight-bearing with crutch support is advised. To counteract the effects of prolonged disuse atrophy, physiotherapy is started during the post-op stage involving electrical stimulations to quadriceps muscles. To improve patellar mobility and avoid knee stiffness, vigorous patellar mobilization is necessary in all directions.
Even with limited knee motion due to pain and immobility, maintaining patellar mobility throughout the recovery period is essential for optimal outcomes. Early passive range-of-motion exercises are initiated by the therapist, focusing on achieving full knee extension and gradually increasing knee flexion over time. During the initial four to five weeks, active extension of the knee is prohibited for letting the tendon heal. During the initial stage of the rehabilitation phase, flexion of the knee is advised by the surgeon which is done actively by the patient himself.
Most surgeons begin to increase knee flexion exercises more aggressively around week 5, which may also include active knee extension exercises. Aquatic therapy can expedite the initiation of active knee extension protocols. By the sixth postoperative week, most surgeons aim to progressively unlock the knee brace to permit ambulation. By the sixth or eighth postoperative week, the goal is to achieve a range of motion of 0 to 120 degrees.
Clinical Importance
The patient is positioned prone for the Nachlas examination. The examiner flexes the patient’s knee until the heel reaches the buttock. If this action causes pain in the front of the thigh, it may suggest compression or irritation of the femoral nerve. But if the discomfort is in the lower back or buttocks, it might be somewhere else.
The test can be performed as the patient lies in a side-lying position. Then the therapist extends the limb, by standing backward to the patient. This technique is also done when the knee is in flexion. Flexion of the knee joint coupled with extension of the hip joint induces traction on the femoral nerve.
Consequently, pain emanating from the anterior thigh region may signify pathology at the L3 nerve root level, while symptoms localized to the medial tibial area may point towards an L4 nerve root compromise. During this maneuver symptoms may be observed on the contralateral side of the limb that signify contralateral radiculopathy.
Rectus Femoris Muscle Pain
In Rectus Femoris the pain can be caused by:
- Strains: Overstretching or tearing of the muscle fibers, often due to sudden movements or overuse.
- Contusions: Bruises caused by impact to the muscle.
- Tendinitis: Inflammation of the tendon that connects the muscle to the bone.
Symptoms :
- Anterior thigh pain
- Swelling
- bruising Difficulty with gait (walking/running)
- Muscle weakness
- Tenderness
Examination of Rectus Femoris Muscle
To distinguish mild traumas or restrict the size of a lesion, manual clinical evaluation is insufficient. X-rays are a useful diagnostic tool for peri-pubertal patients, enabling the identification of apophyseal detachments, which are characteristic of this developmental stage. Additionally visible are intramuscular calcifications of the quadriceps muscle.
To distinguish mild traumas or restrict the size of a lesion, manual clinical evaluation isn’t sufficient. X-rays can identify age-related apophyseal detachments and intramuscular calcifications in the quadriceps.
Owing to the elevated costs, magnetic resonance imaging remains a secondary imaging choice. Ultrasound imaging is a cost-effective modality that provides superior visualization of soft tissues and allows for dynamic assessment.
FAQs
Which four muscles make up the quadriceps?
The muscles located on the anterior surface of the thigh are collectively known as the quadriceps.The rectus femoris, vastus lateralis, vastus intermedius, and vastus medialis are the four separate muscles that make up this structure. They are in charge of extending the leg and facilitating motions like walking and leaping.
What does the Rectus Femoris muscle actually do?
For exercises like jumping, sprinting, and kicking, knee extension is essential because it straightens the knee joint.
It also Assists in pulling your thigh closer to your torso, which is known as hip flexion.
Which Rectus Femoris muscle injuries are most common?
Strains: Excessive stretching or tearing of the muscular fibers, frequently brought on by overuse or abrupt movements. Mild to severe strains are possible.
Contusions: Bruises brought on by a forceful blow to the muscle.
What signs of an injury to the rectus femoris muscle are present?
Bruising and swelling
Having trouble running or walking
Weakness or discomfort in the muscles
Painful thigh
The Rectus Femoris muscle is found where?
It is the quadriceps muscle that is nearest to the skin’s surface, making it the most superficial.
It extends from the hip bone (pelvis) to the kneecap (patella) down the front of your leg.
How can I avoid injury to my Rectus Femoris muscles?
Warm up correctly: To improve blood flow and prime the muscles, do dynamic stretches before to engaging in any physical activity.
Strength training: To increase muscular balance and stability, do exercises that focus on the hamstrings and quadriceps on a regular basis.
Training correctly: To prevent overtaxing your muscles, gradually increase the length and intensity of your sessions.
Rest and recuperation: Give your muscles enough time to rest in between exercises.
Which test is used for Rectus Femoris muscle?
The Kendall Test, also known as the modified Thomas Test, is a commonly employed orthopedic maneuver designed to assess the length and flexibility of the rectus femoris muscle within the quadriceps group.
To perform this test:
The patient is positioned supine with both legs initially extended off the edge of the examination table.
Subsequently, the patient is instructed to actively flex one knee towards their chest while maintaining this position.
References:
- Rectus femoris muscle. (2024, December 21). In Wikipedia. https://en.wikipedia.org/wiki/Rectus_femoris_muscle
- Quadriceps femoris muscle. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/the-quadriceps-femoris-muscle
- Rectus Femoris, Physio Pedia, https://www.physio-pedia.com/Rectus_Femoris

One Comment