Rood’s Approach
Introduction
Margret Rood created the neurophysiological and developmental therapeutic method known as “Rood’s approach” to enhance muscular tone, including both flaccidity and spasticity.
Rood’s technique was created specifically for people with motor control issues and is based on the physiological reality that sensory input elicits the optimal muscle response. Developmental sequences are used, i.e., practicing sensory-motor response until learning is accomplished and progressing from lower to higher levels. The laws of sensory input are as follows:
- a quick stimulus results in synchronous movement output;
- a quick stimulus repeated quickly results in a sustained reaction; and
- a sustained response results from sustained sensory input.
- and a slow, repeated, and rhythmic stimulus lowers the tone of the muscular response.
Furthermore, we may activate the vestibular receptors by bending the neck sideways, extending it, rotating it, and flexing it. Symmetric and asymmetrical tonic neck reflexes are even more effective for producing tone in the flexors and extensors.
Rood’s strategy was predicated on four fundamental ideas:
- Muscle tone normalization by sensory stimulation.
- Pattern of ontogenetic development.
- Repeating.
- Purposeful motion.
- Proprioceptive receptors, exteroceptive receptors, vestibular receptors, and special sense organs are the four types of receptors that may be triggered to obtain the correct muscle response, according to Rood.
According to Rood’s method, sensory input results in;
- Trophic alteration is caused over time by axoplasmic flow in neuronal processes as well as an immediate effect by transmission of nerve impulses.
- It is feasible to achieve the intended muscle response by stimulating the receptor in a way that either facilitates or inhibits it.
Fundamentals
- Making use of regulated stimulation of the senses.
- The application of ontogenic developmental sequences was advised by Rood.
- Rood claims that because sensory-motor control is developmentally based, the therapist must first determine the patient’s present developmental stage before attempting to raise the patient’s control to the next level.
- the use of a task to prompt a deliberate answer.
- Normalization of tone and muscular responses: The fundamental idea of the Rood method is to use the right sensory cues to evacuate the correct muscle response.
- Developmentally based sensor motor control is used.
- It is thought that the muscular reactions of synergists, antagonists, and agonists are automatically programmed by a goal or plan.
- Practice and repetition are essential for learning and motor control.
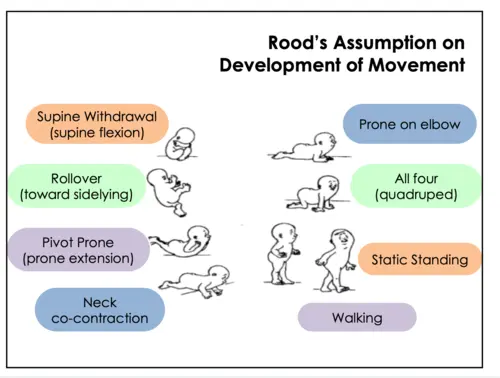
The pattern of ontogenic development
These typical developmental patterns served as the foundation for the therapy. These patterns may be utilized to either facilitate or inhibit by situating oneself in these patterns; they also have positive effects when linked with occupational involvement.
Supine withdrawal, often passive flexion, is the whole flexion reaction directed at the T10 spinal level. The anterior surface of the body is shielded in this protective position by the flexion of the neck and the crossing of the arms and legs. This design is advised for those whose extensor tone predominates.
Rollover (to the side): Rollover engages the lateral trunk musculature and is a movement pattern for the extremities. For those who are dominated by tonic reflex patterns in the supine position, it is recommended.
The pivot-prone posture, also known as prone extension, requires the neck, shoulders, trunk, and lower extremities to be fully extended. It is a pattern of both motion and stability. It is essential in laying the groundwork for the extensor muscles’ stability when standing.
Neck co-contraction, also known as co-innervation, is believed to engage the neck’s deep tonic extensors as well as flexors. In addition to promoting stability and extraocular control, this posture generates a tonic labyrinthine righting reaction.
On elbows (prone on elbows): Applying weight to the elbows strains the muscles in the upper trunk, which affects how stable the scapular and glenohumeral areas are. Inhibitory to the symmetrical tonic neck reflex is this stance.
All fours (quadruped posture): This position brings the lower extremities and trunk into a coordinated pattern of contraction. The shifting of weights is a prelude to equilibrium reactions.
Standing motionless: Taking a balanced stance. Higher-order neural integration is brought about by this posture, including balance and righting reflexes.
Walking: The stance phase, push-off, swing, heel strike, and stride length are all included in walking. It’s a complex procedure that calls for precise movement patterns from many body regions, including changing one’s weight.
The two methods in Rood’s approach are as follows:
Facilitating methods to enhance the tone of weak muscles
Tactile stimulation: Light stroking and quick brushing
Fast brushing is the process of using a soft paintbrush or battery-operated brush to quickly brush hair or skin over a muscle.
The skin of the muscle that has to be worked is where brushes are always pointed. One type of high-intensity stimulation is fast brushing. The non-specific impact lasts for a maximum of thirty to forty minutes following stimulation. Precautions include placing pressure over the pinna of the ear (stimulation of the vagus nerve may impact CVS), over the posterior main rami of L1, L2, and S4 (used for incontinence patients) (may generate voiding).
Light touch can be applied using cotton swabs or fingertips. The extra fugal motor system’s facilitation often stimulates low threshold receptors.
- A and C icing are examples of thermal facilitation
A: Icing: rapidly apply ice cubes to induce a reflexive retreat that mimics light touch
C stands for icing or elevated stimulus threshold. Ice cubes are applied to the dermatome region or the muscular belly and pushed for 15 to 20 minutes. Warnings: the same as when brushing
Additionally, it is hypothesized that icing and brushing have reciprocal effects. Therefore, it is advantageous to stimulate the unaffected side of hemiplegic patients before stimulating the affected side.
A quick light stretch is a low threshold stimulation that causes the stretched muscle to have a phasic reaction. Quick stretch has an instant impact. To facilitate the muscle, tapping over a tendon or muscle belly is helpful.
Pressure: Applying pressure on the muscular belly stretches the muscle spindles, causing a stretch reaction.
Excessive joint compression enables the surrounding muscles to co-contraction. It is used on the bone’s longitudinal axis. Weight-bearing postures or manual compression can be used to administer it. Prone on hand, for instance. Force is applied to the prominence of the bones.
Olfactory and gustatory stimuli are examples of approaches used as facilitators to specialize certain senses.
Inhibitory methods for lowering spastic muscle tone
A joint approximation is another name for light joint compression. Utilized to suppress tone in muscles that are hypertonic.
Slow stroking: Applying light pressure to the posterior rami slowly but firmly inhibits the tone. After three to five minutes, the patient starts to relax.
The patient can be rocked gently or gently rotated from a supine posture to a side-lying position. The state of sustaining body temperature by encircling the intended area to be confined is known as neutral warmth. It’s finished in ten to twenty minutes.
The heat that is higher than body temperature is employed as a rebound effect and this is known as neutral heat. Through the receptors there, pressure applied to a muscle’s insertion inhibits that muscle.
Resuming a lengthier posture for a duration varying from a few minutes to many weeks causes the muscle spindle to revert to its original length. A long-held stance throws off the equilibrium between the agonistic and hostile tones.
Low threshold GTOs can be employed to block the agonists by unresisted contraction; this would assist the antagonists in return.
The foundation of Rood’s approach
Rood’s four fundamental ideas are:
Muscles of mobility and stability (phasic and tone).
As to Rood’s methodology, muscles may be classified into two groups.
Deep, slowly oxidizing muscles called tonic muscles are in charge of stabilizing joints.
Phasic muscles are often single-joint muscles that are responsible for skillful motions. They are superficial, quickly glycolytic, and rapidly fatigued.
The Ontogenic Sequence
Rood two categories of ontogenic sequences were explained.
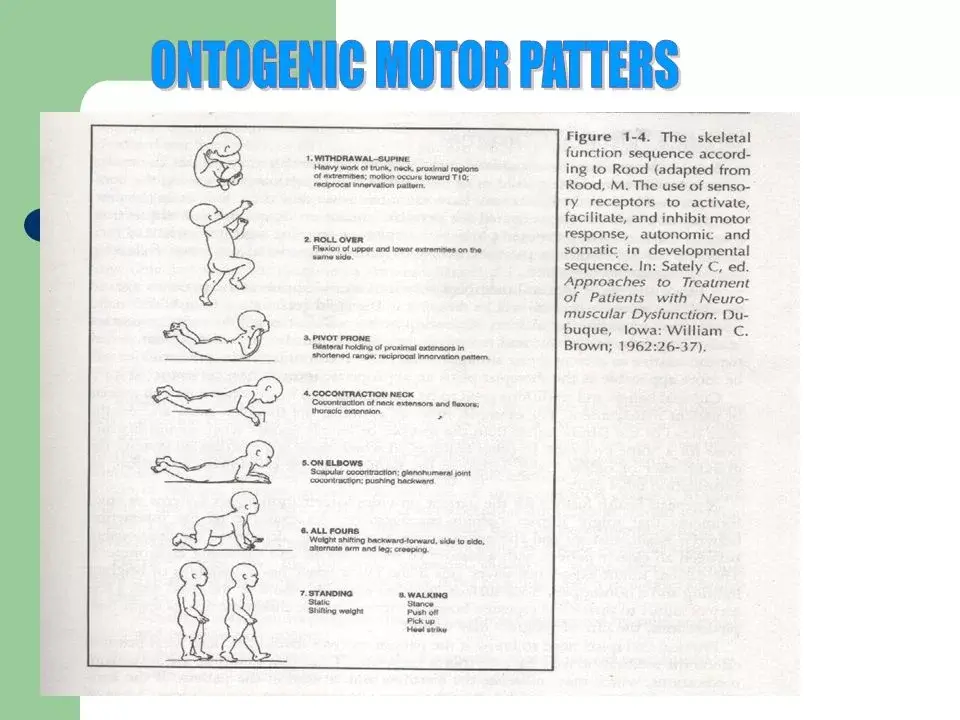
The order of motor development Eventually, the cycle of motor development results in proficient and exquisitely synchronized motions. The supine withdrawal, roll over, pivot prone, and roll over are the ontogenic motor patterns. Contraction of the neck. v. prone on the second elbow. Fourfold vii. Position viii. Strolling
Rood additionally used the ideas of light and heavy labor to group these patterns into the following four phases: i. Reciprocal innervations or mobility: It is essentially a reflex controlled by the spinal and supraspinal centers, and it exhibits near mobility. It involves pivot prone, rollover, and supine withdrawal. ii. Contraction or stability:
It is described as the simultaneous contraction of agonists and antagonists, which cooperate to support and preserve the body’s posture. It consists of standing, quadruped, neck co-contraction, pivot prone, and prone on the elbow. iii. Mobility is the movement of proximal limb segments while the distal ends of the limbs stay stationary on the support base.
Mobility is stability over stability. It involves quadrupedal weight shifting on elbows, as well as to-and-fro rocking, which can eventually be advanced to direction-changing crawling. iv. Distal mobility with proximal stability, also known as skillful work, is characterized by the emphasis on the movement of the body’s distal parts in a precisely coordinated pattern, which calls for control at the highest cortical level.
b. The order of vital functions
Well-articulated speech is ultimately the result of the important function sequence. The ontogenic patterns are i—inspiration. Chewing and swallowing food; phonation; swallowing liquids; expiration; and sucking. vii. Conversation.
Suitably stimulated senses
Rood made use of the receptiveness of anterior horn cells by stimulating the senses.
Rood used sensory stimulation to exploit the responsiveness of anterior horn cells. To elicit the intended muscle response, Rood claims that four different types of receptors can be activated: i. Vestibular receptors ii. Exteroceptive receptors iii. Proprioceptive receptors IV. Particular sensory organs.
Autonomic nervous system manipulation
Rood’s approach also includes activation of the autonomic nervous system. The stimulation’s varying frequencies and intensities dictate whether the system—the parasympathetic or sympathetic—will become active.
Rood emphasized that patients who are hypertonic, hyperkinetic, or hyperexcitable should get stimulation of their parasympathetic nervous system, whereas hypotonic somnolent patients should receive activation of their sympathetic nervous system. Rood suggested that individuals with motor disorders might benefit from the modulation of these stimuli.
The following are examples of stimuli that activate the sympathetic nervous system: frosting, disagreeable tastes or fragrances, brief, sharp spoken instructions, bright lights that flash, rapid motion, and rhythmic music.
Nervous System Parasympathetic Stimuli include lightness, soft music, pleasant odors, touch on the palms of hands, soles of feet, upper lip, or abdomen. They also consist of rolling, shaking, and petting the skin over the paravertebral muscles in a steady, rhythmic, repeating manner.
Techniques
- Faciliatory Technique
- Inhibitory Technique
Postural tone is improved by the employment of functorial approaches during a goal-directed activity. Three types of motions are employed to encourage or support movement response: vestibular, proprioceptive, and tactile.
- Light touch
- brushing
- Fast stroking
- Stretching
- Positioning
- resistance
- Joint Compressions
Inhibitory Techniques are just opposite to faciliatory movement. it is usually used to maintain the muscle tone.
- Neutral
- Warmth
- Gentle stroking
- Light joint compression
- Pressure
Roods Approach For incomplete nerve injury roods facilitation techniques are used in treating incomplete nerve injury. the pattern of facilitations include
- Quick Brushing
- Quick icing
- Vibration
- Tapping
- Quick Brushing
applied three to five times, then paused for thirty seconds before repeating. The skin covering the muscles should have the same root supply as the dermatomes and myotomes. Its effects might linger for up to 20 minutes. Swift icing right after brisk brushing. Its impact lasts for up to fifteen minutes.
Vibration
At the musculotendinous junction of stretched muscle or the muscular belly, vibrations are applied. There are 100–200 hertz vibrations at high frequencies. For up to ten minutes, the tonic vibration reflex impact facilitates muscular contractions.
Tapping
Apply three to five gentle taps with little pressure on the muscle belly or tendon. activation of the main ends of muscle spindles, which causes the muscle to be reflexively facilitated by the monosynaptic reflex
The most crucial component of Rood’s neurophysiologically based approach is pertinent physiology, an area that was not well investigated during her lifetime. While the full Rood method is not yet employed, certain of its strategies are widely used in therapeutic settings.
Current scientific evidence shows Rood’s approach has various valid components that can be justified as valid and viable. A therapist may get more effective results if they use it with a physiological base.
Basic concepts
Rood’s four basic concepts are;
- Muscles of mobility and stability (phasic and tonic).
- Order of motor development.
- appropriate stimulation of the senses.
- The autonomic nervous system is being manipulated.
- Its function in patients with strokes
- Rood’s method is important for enhancing the capacity for self-care that is autonomous. This remarkable improvement might be attributed to the two parts of Rood’s therapy that are;
- Proprioceptor, exteroceptor, and vestibular stimulation facilitation or inhibition stimulate the cerebral level and result in motor recovery.
- In addition to the skeletal muscles, Rood’s technique also includes stimulation, which may be used to increase the motor activity of important organs.
- Rood’s method helps patients recover from strokes by using a variety of workouts and activities. Repeating motions and activating various body areas are the focus of these workouts. People can improve their ability to take care of themselves on their own by engaging in meaningful activities and stimulating their senses. These kinds of activities have also been demonstrated in other trials to help stroke patients’ motor abilities. For the arms, they might need to attempt to open a container or wash off a table. For the legs, they may need to kick a ball or get up from a seated posture. therefore it can stop several illnesses and deaths, such as contractures, pneumonia, decubitus ulcers, and deep vein thrombosis.
FAQs
What is Rood’s approach?
Rood’s method uses rolling and mild joint compressions to prevent aberrant hypertonia while stimulating exteroception and proprioception to produce muscle tone. Exteroceptor stimulation tends to activate the sympathetic nervous system, which then activates the motor system.
What are the principles of Rood?
Normalization of tone, ontogenic developmental sequence, intentional movement, and practice or repetition are the cornerstones of the Rood method.
What is the Rood and Brunnstrom approach?
To start the proper motor pattern development, Rood’s methods concentrate on the basic reflexes that are triggered by sensory impulses that reach the targeted sensory receptors. The strategies developed by Brunnstrom expand on the synergies to elicit the affected limbs’ involvement.
What is the Rood approach for hypotonia?
A fundamental tenet of the Rood method is the normalization of tone through the use of sensory inputs. Normalizing muscular tone is aided by the facilitation and inhibition of muscle action by sensory stimuli. Tactile stimulation can improve muscle tone in individuals with hypotonic disorders, claims Linkous et al.
What are inhibitory techniques?
Slow rocking, slow anterior-posterior, slow horizontal, slow vertical, and slow linear motions can all lead to total body inhibition. Crawling, rolling patterns, and a rocking pattern on extended elbows can all lead to total body facilitation.
References
- Rood Approach. (n.d.). Physiopedia. https://www.physio-pedia.com/Rood_Approach
- Clinic, M. P. Rood’s Approach – Mobile Physiotherapy Clinic. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/roods-approach/
- Rood’s Approach: Neurology Physiotherapy Treatment Technique. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/roods-approach-techniqe/
- Roods Approach : Explained. https://www.reboundsphysiotherapy.com/post/roods-approach-explained