Ulnar Collateral Ligament
Introduction
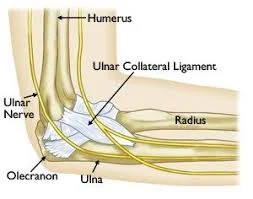
The ulnar collateral ligament (UCL) is a strong band of tissue located on the inner side of the elbow, connecting the humerus (upper arm bone) to the ulna (one of the forearm bones). It provides stability to the elbow joint, particularly during activities involving throwing or overhead motions.
UCL injuries are common in athletes, especially baseball pitchers, often requiring rest, physical therapy, or in severe cases, surgical repair like Tommy John surgery. For athletes, coaches, trainers, and medical professionals who provide treatment for people who participate in these kinds of activities, it is critical to understand the structure and function of the ulnar collateral ligament.
Structure of the Ulnar Collateral Ligament
The three separate bands that make up the complicated ulnar collateral ligament (UCL) each have a unique purpose and location of attachment.
Between the medial epicondyle of the humerus, a bony elevation on the inside of the upper arm bone, and the sublime tubercle of the ulna, a little bony projection on the inside of the forearm bone, lies the anterior bundle, the largest and most significant of the three bands.
During overhead throwing motions, this bundle is in the role of preventing the elbow joint from experiencing excessive valgus (outward) stress.
From the medial epicondyle of the humerus to the olecranon process of the ulna (the bony protuberance at the elbow’s tip), the posterior bundle lies behind the anterior bundle. During overhead throwing actions, this bundle gives the elbow joint more stability.
The oblique bundle, which lies between the anterior and posterior bundles, is the smallest of the three bands. It extends from the ulna, just below the sublime tubercle, to the medial epicondyle of the humerus. When the elbow joint is under valgus or varus (inward) tension, this bundle aids in keeping it stable.
Generally speaking, the ulnar collateral ligament is a robust, thick band of tissue that gives the elbow joint vital support when throwing high. This ligament can sustain severe injuries that may need to be repaired or rebuilt surgically.
Functions of the Ulnar Collateral Ligament
A thick band of tissue called the radial collateral ligament (RCL) connects the annular ligament—a ring-shaped structure that encircles the head of the radius, one of the two forearm bones—to the lateral epicondyle of the humerus, a bony prominence on the outside of the upper arm bone. During movements involving varus (inward) tension, the elbow joint is stabilized by the radial collateral ligament.
Preventing excessive varus stress on the elbow joint is the main purpose of the radial collateral ligament. When the elbow is struck on the outside or during specific throwing actions, the forearm is pulled inside towards the body, causing this kind of tension. The radial head is held in place by the radial collateral ligament, which also keeps it from sliding out of the joint, which could result in discomfort, instability, and long-term harm.
The radial collateral ligament’s primary function is to stabilize the elbow joint; it also helps with other movements, like gripping and lifting objects. It provides general stability and support in the elbow by cooperating with other ligaments and muscles.
Blood supply of the Ulnar Collateral Ligament
Numerous arteries and branches that emerge from the brachial, ulnar, and interosseous recurrent arteries supply the ulnar collateral ligament.
The anterior ulnar recurrent artery, which emerges from the ulnar artery, supplies blood to the anterior band of the ulnar collateral ligament. This artery supplies blood to the anterior part of the ulnar collateral ligament as it passes anteriorly along the medial aspect of the elbow.
The posterior ulnar recurrent artery, which likewise emerges from the ulnar artery, supplies blood to the posterior band of the ulnar collateral ligament. The posterior part of the ulnar collateral ligament receives blood supply from this artery, which runs posteriorly along the medial edge of the elbow.
The interosseous recurrent artery, which emerges from the common interosseous artery, supplies blood to the transverse band of the ulnar collateral ligament. This artery supplies blood to the transverse section of the ulnar collateral ligament and crosses the elbow joint obliquely.
These arteries are joined by some anastomoses, or connections, which give the ulnar collateral ligament collateral circulation. Blood can still reach the ulnar collateral ligament through other pathways even if one vessel is blocked due to these anastomoses.
Therefore, we can generally state that the ulnar collateral ligament’s blood supply is essential to preserving its integrity and avoiding injury. An inadequate blood supply can cause ligament degeneration and weakening, which raises the possibility of injury when throwing.
Injuries of the Ulnar Collateral Ligament
Athletes who play throwing sports, like baseball, softball, and javelin throwing, frequently get ulnar collateral ligament (UCL) injuries. These activities can cause ulnar collateral ligament injuries because of the repetitive and powerful motions they require, which can place a lot of strain on the elbow joint. The following activities can result in injury to the ulnar collateral ligament:
- Throwing: The ulnar collateral ligament may be overstressed by frequent, high-velocity ball throwing, which may result in minor tears or whole ruptures. Because they make so many throws throughout a game, pitchers in softball and baseball are especially prone to ulnar collateral ligament injury.
- Inadequate technique: Ulnar collateral ligament injuries can also result from poor throwing mechanics, such as employing too much arm and not enough body. The elbow joint must bear additional strain when the correct technique is not applied, which raises the possibility of injury.
- Overuse: Ulnar collateral ligament injuries can also result from excessive elbow joint use without adequate rest and recuperation. Regular throwers who don’t give themselves enough time to relax and heal are more likely to have an injury to their ulnar collateral ligament.
- Sudden trauma: Another cause of ulnar collateral ligament injuries is a sudden impact or trauma to the elbow joint. For instance, the ulnar collateral ligament may sustain severe harm if a baseball strikes the elbow joint directly.
- Insufficient warm-up: The risk of ulnar collateral ligament injuries can also be raised by improperly warming up before throwing activities. A good warm-up lowers the chance of injury by preparing the muscles and joints for the strain of throwing.
We might conclude that because throwing sports require repetitive and strong actions, ulnar collateral ligament injuries are frequently observed in athletes who participate in them. The likelihood of ulnar collateral ligament injuries can be decreased with the use of proper technique, rest and recuperation, and warm-up exercises.
Symptoms of the Ulnar Collateral Ligament Injury
Depending on how severe the injury is, ulnar collateral ligament symptoms can change. These are a few typical symptoms:
- Elbow pain: Elbow joint discomfort is the most typical sign of an injury to the ulnar collateral ligament. Throwing and other activities that put stress on the ulnar collateral ligament can exacerbate the discomfort, which may be felt on the inside of the elbow.
- Swelling: Injury to the ulnar collateral ligament may result in swelling, stiffness, and restricted range of motion in the elbow joint.
- Weakness: An injury to the ulnar collateral ligament may result in weakness in the affected arm, which makes it difficult to carry out strength-demanding activities like throwing a ball.
- Tingling or numbness: Numbness or tingling in the fingers or hand may occasionally result from an injury to the ulnar collateral ligament.
- Instability: An elbow joint that is unstable due to severe ulnar collateral ligament injuries may feel loose or wobbly.
It is important to remember that not all injuries to the ulnar collateral ligament result in symptoms right away. Not identifying to them, some athletes may keep playing through ulnar collateral ligament injuries, which can result in more difficulties and injuries. You should get medical assistance right away if you experience any of these symptoms or think you might have an ulnar collateral ligament injury.
Diagnosis of the Ulnar Collateral Ligament Injury
A physical examination, imaging studies, and a study of the patient’s symptoms and medical history are usually used to diagnose an ulnar collateral ligament injury. To diagnose an injury to the ulnar collateral ligament, follow these steps:
- Physical examination: The doctor will start by checking for swelling, soreness, and instability in the elbow joint. The affected arm’s strength and range of motion may also be evaluated through a variety of tests.
- Imaging testing: The doctor may prescribe imaging tests like X-rays, MRIs, or ultrasounds to confirm the diagnosis and assess the extent of the injury. These examinations can assist in detecting any ligament rips, bone fractures, or other elbow joint injuries.
- Medical history and symptoms: Inquiring about the patient’s medical history, including any prior diseases or injuries that might have caused the ulnar collateral ligament injury, is another thing the doctor will do. Along with the onset and duration of symptoms, they will also ask about any activities that may have contributed to or caused the pain.
The doctor can diagnose a patient and provide a suitable treatment plan based on the findings of these tests and examinations. In certain situations, reconstructing or repairing the injured ulnar collateral ligament may need surgery. For others, conservative measures like physical therapy, rest, and anti-inflammatory drugs could be enough to control symptoms and encourage recovery.
Treatment of the Ulnar Collateral Ligament Injury
Examination test
The Valgus stress test
A physical examination technique called the valgus stress test is used to evaluate how stable the elbow joint’s ulnar collateral ligament (UCL) is. An essential ligament that aids in stabilizing the elbow joint during throwing and other repeated arm motion activities is the ulnar collateral ligament.
The patient is positioned with their forearm twisted outward and their elbow bent at a 20–30 degree angle to do the valgus stress test. One hand is then placed on the patient’s hand or wrist, and the other is placed on the outside of the elbow joint, just above the wrist.
The elbow joint is then forced outward and away from the body by the examiner using a medial force. The ulnar collateral ligament, which runs down the inside of the elbow joint and aids in limiting excessive outward movement of the joint, is stressed by this tension.
The examiner will feel a firm end-point if the elbow joint resists this medial force and the ulnar collateral ligament is healthy. This shows that the ulnar collateral ligament is giving the joint enough support.
The elbow joint will move too outward, though, if the ulnar collateral ligament is injured or ripped, and the examiner will notice a soft end-point or a space between the bones. This suggests that there may be injury to the ulnar collateral ligament, which is not giving the joint enough stability.
The valgus stress test is frequently used to evaluate injury to the elbow joint’s ulnar collateral ligament in combination with other physical examination techniques and imaging testing. Treatment may involve rest, physical therapy, bracing, or surgery depending on the degree of the injury.
Conservative treatment
Rest, physical therapy, and bracing are commonly used conservatively to treat ulnar collateral ligament problems. Conservative treatment aims to strengthen and stabilize the elbow joint, lessen discomfort and inflammation, and encourage recovery.
Rest: When it comes to ulnar collateral ligament injuries, rest is crucial to the healing process. Throwing and repetitive arm motions are two activities that patients may need to avoid since they put stress on the elbow joint. Elbow rest lowers the chance of further injury and promotes healing of the affected ligament.
Physical treatment: To assist patients in regaining elbow joint strength and range of motion, physical therapy is frequently advised. Stretching, strengthening, and range-of-motion exercises are all possible. Enhancing neuromuscular control and proprioception through physical therapy can also lower the chance of further injuries.
Bracing: To give the elbow joint stability and support while it heals, a brace or splint may be advised. A brace may lessen discomfort and inflammation by limiting excessive joint mobility.
Nonsteroidal anti-inflammatory medicines (NSAIDs): To help lower pain and inflammation, NSAIDs like naproxen or ibuprofen may be prescribed. These drugs can help reduce pain and swelling, but they should be used carefully because they might have adverse effects like irritated stomachs.
Conservative treatment may not always be successful in treating injuries to the ulnar collateral ligament, especially when there are extensive tears or ruptures. Surgery may be required in these situations to rebuild or repair the injured ligament.
Physiotherapy treatment
Exercises and manual therapy techniques are commonly used in physiotherapy treatment for ulnar collateral ligament injuries to help increase the range of motion, decrease discomfort and inflammation, and strengthen and stabilize the elbow joint. In addition to the patient’s unique needs and objectives, the extent and location of the injury will determine a specific path of treatment.
The following are some typical physiotherapy methods for ulnar collateral ligament injuries:
Manual therapy: This includes manual methods including stretching, joint mobilization, and massage to assist ease pain and increase elbow range of motion.
Strength training: Since strengthening exercises help to regain elbow stability and strength, they are a crucial component of ulnar collateral ligament rehabilitation. Elbow flexion, extension, wrist curls, and grip strengthening exercises are a few possible exercises.
Exercises for range of motion: Range of motion exercises are used to increase elbow joint flexibility and mobility. These could be passive range-of-motion exercises or stretching techniques carried out with a therapist’s help.
Exercises for neuromuscular control: These are intended to help patients become more adept at controlling their hand and arm movements. This may lessen the possibility of further injuries.
Bracing or taping: During rehabilitation, bracing or taping may be utilized to give the elbow joint more stability and support.
Modalities: To help reduce elbow joint discomfort and inflammation, modalities like electrical stimulation, ultrasound, or cold may be applied.
Thus, we may conclude that the goal of physiotherapy for ulnar collateral ligament injuries is to encourage healing, lessen discomfort and inflammation, and provide elbow joint strength and stability again. Many people can resume their prior level of activity without surgery with the right care and therapy.
Risk factors
The band of tissue that joins the inside of the elbow to the upper arm bone is called the ulnar collateral ligament, or UCL. It is in the role of keeping the elbow joint stable when throwing or performing repetitive overhead motions. However, other risk factors can make ulnar collateral ligament injuries more likely. Among these are:
- Overuse: The ulnar collateral ligament can be overstressed by repetitive overhead motions, like throwing a baseball or playing tennis, which raises the risk of injury.
- Poor technique: Injuries to the ulnar collateral ligament can also result from using incorrect throwing or hitting techniques.
- Age: Adolescent and young adult athletes who are still growing and developing are more likely to sustain ulnar collateral ligament injuries.
- Gender: Male athletes are more likely than female athletes to sustain ulnar collateral ligament injuries.
- Prior injury: Future ulnar collateral ligament injuries may be more likely in people with a history of elbow injuries or ulnar collateral ligament injuries.
- Muscle imbalances: The ulnar collateral ligament may be subjected to additional strain and injury risk if there is weakness or imbalance in the shoulder, arm, or forearm muscles.
- Joint laxity: An increased risk of ulnar collateral ligament injuries may result from some people’s naturally loose or unstable joints.
- Genetics: A person’s vulnerability to ulnar collateral ligament injuries may be heightened by specific genetic factors.
By strengthening muscles, avoiding overuse, and avoiding repetitive motions, people can prevent ulnar collateral ligament injuries by being aware of these risk factors.
How may Ulnar Collateral Ligament Injury risk be reduced?
The following actions can help prevent injuries to the ulnar collateral ligament:
- Correct Technique: The ulnar collateral ligament can be less stressed by using appropriate throwing or hitting techniques. Trainers and coaches can teach athletes the right ways to avoid injuries.
- Strengthening Exercises: You can lessen the strain on the ulnar collateral ligament by strengthening your shoulder, arm, and forearm muscles. These muscles can be strengthened with exercises like tricep extensions, bicep curls, and shoulder external rotation.
- Rest and Recovery: You can lower your risk of overuse injuries by taking a break between practices and games. Additionally, after practices and competitions, athletes should take some time to stretch and cool down.
- Gradual Progression: To prevent abrupt increases in the strain on the ulnar collateral ligament, athletes should progressively increase the frequency and intensity of their workouts.
- Proper Equipment: The ulnar collateral ligament can be less stressed by wearing the right gear, such as elbow sleeves, gloves, and padding.
- Cross-training: By providing the ulnar collateral ligament with a respite from repetitive motions, engaging in other sports or activities can help lower the risk of overuse injuries.
- See a Physician: Before resuming sports, athletes with a history of elbow injuries, such as ulnar collateral ligament injuries, should see a physician to make sure they are fully recovered and prepared to compete.
These precautions can help athletes stay healthy while playing sports and engaging in other activities by lowering their risk of ulnar collateral ligament injuries.
FAQ
The ulnar collateral ligament (UCL) is what?
The inside of the elbow joint contains a ligament called the ulnar collateral ligament, which aids in stabilizing the joint when throwing and performing other overhead movements.
What leads to injuries to the ulnar collateral ligament?
Repetitive overhead motions that put stress on the ligament, like throwing a baseball or softball, are frequently the cause of ulnar collateral ligament injuries. They may also result from abrupt elbow trauma.
What features define an injury to the ulnar collateral ligament?
An injury to the ulnar collateral ligament may manifest as inside elbow pain, swelling, reduced range of motion, and a sense of instability in the joint.
How can injuries to the ulnar collateral ligament be identified?
A physical examination and imaging tests like MRIs or X-rays are usually used to diagnose ulnar collateral ligament injuries.
How are injuries to the ulnar collateral ligament treated?
Injuries to the ulnar collateral ligament can be treated with rest, ice, physical therapy, and occasionally surgery.
Is it possible to avoid ulnar collateral ligament injuries?
The use of appropriate techniques, strengthening exercises, rest and recovery, gradual progression, appropriate equipment, cross-training, and medical advice can all help prevent ulnar collateral ligament injuries.
References
- Patel, D. (2023b, August 14). Ulnar Collateral Ligament – Anatomy, structure, function. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/ulnar-collateral-ligament/

One Comment