Triangular Fibrocartilage Complex (TFCC) Injury
What is Triangular Fibrocartilage Complex Injury?
The Triangular Fibrocartilage Complex (TFCC) injury involves damage to the cartilage and ligaments on the ulnar side of the wrist, which provide stability and cushioning. It commonly occurs due to falls on an outstretched hand, repetitive wrist motions, or degenerative wear.
Symptoms include wrist pain, weakness, and clicking sensations, especially with rotation or weight-bearing activities. Treatment ranges from rest and bracing to physical therapy or, in severe cases, surgery.
Numerous factors, such as traumatic events like falls onto an outstretched hand, violent twisting motions, or direct strikes to the wrist, can result in TFCC injuries. Additionally, they may develop gradually as a result of deterioration over time and recurrent trauma. Athletes, especially those participating in weight-bearing or repetitive wrist-moving sports, and people working in jobs requiring a lot of wrist use, are more likely to sustain TFCC injuries.
Ligaments, cartilage, and tendons make up the triangular fibrocartilage complex (TFCC), a level of arrangement in the wrist that offers support and stability. From tears to strains, TFCC injuries can result in wrist pain, instability, and restricted range of motion.
Treatment options include rest, splinting, physical therapy, and in certain situations, surgery. They can be caused by trauma or slow wear and tear. For TFCC injuries to be correctly diagnosed and treated, medical advice is crucial.
Clinically relevant Anatomy:
Injuries to the triangular fibrocartilage complex (TFCC) affect wrist structures that are essential to its stability and functionality. The following clinically significant elements make up the TFCC, which is situated on the ulnar side of the wrist:
The specialized cartilage known as the triangular fibrocartilage lies between the wrist’s carpal bones and the ulna, one of the forearm bones.
- The Ulnar Collateral Ligament (UCL) stabilizes the wrist joint by joining the ulna to the carpal bones.
- Ulnar Carpal Ligaments: These ligaments, which join the ulna to particular carpal bones, support the integrity of the TFCC as a whole.
- The fibrous substance known as the articular disc serves as a cushion between the carpal and ulna bones, allowing for shock absorption and smooth movement.
- The Extensor Carpi Ulnaris (ECU) sheath: The ECU tendon allows wrist movement by passing through the TFCC and encircling the ulna.
- Meniscus Homologue: This structure gives the TFCC more rigidity and support and resembles the meniscus in the knee joint.
Epidemiology:
According to one study, TFCC injuries are more common as people age. The prevalence was 27% in patients 30 years of age or younger and 49% in patients 70 years of age or older, according to the investigators. The prevalence of TFCC injury was similar in patients under 30 years old, according to another study, but it was also similar in patients who experienced ulnar-sided pain as opposed to those who underwent wrist imaging for other reasons. According to this study, not all TFCC injuries result in pain on the ulnar side.
Pathophysiology:
The ulnotriquetral and ulnolunate ligaments, the dorsal and volar distal radioulnar ligaments, the meniscal homolog, the triangular fibrocartilage disc, the extensor carpi ulnaris tendon subsheath, and the ulnocarpal collateral ligament are all anatomically included in the TFCC. The radial side’s triangular fibrocartilage disc attachment to hyaline cartilage is weaker than the bony attachment on the ulnar side.
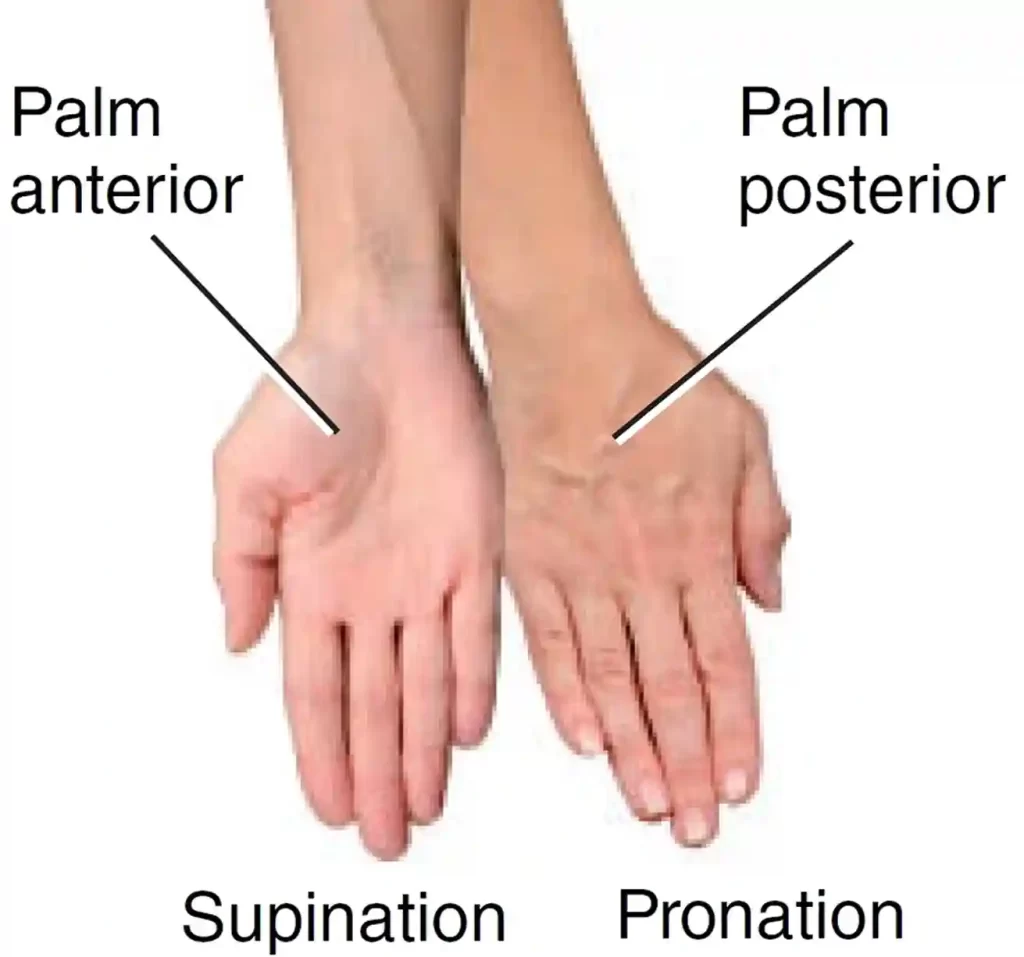
If the ulnar variation is positive, the TFCC may be at risk for harm. When pronating, ulnar variation will rise, and when supinating, it will decrease. It has been demonstrated that slight variations in ulnar length significantly impact the amount of force applied to the ulna. Because the extensor carpi ulnaris depends on the TFCC for movement, any change in its motion could result in anomalous force passing through the TFCC, making it more vulnerable to damage.
Causes of triangular fibrocartilage complex injuries:
Injury to the triangular fibrocartilage complex (TFCC) can result from a number of factors. The following are the etiology (causes) of TFCC injuries:
- Trauma: TFCC injuries may result from unexpected violent collisions or mishaps, such as falls onto an outstretched hand. The TFCC components may sustain tears or strains as a result of direct damage to the wrist.
- Repetitive Strain: Overuse or repetitive wrist motions, as those found in racket sports or other sports, or occupational duties, can eventually lead to TFCC problems.
- Wrist Fractures: Injuries may result from fractures of the ulna or distal radius, which can affect the TFCC indirectly. The TFCC may experience stress or malfunction as a result of the misaligned bones.
- Aging and Degeneration: The TFCC may age naturally or experience wear and tear over time, making it more prone to damage.
- When the ulna bone is comparatively longer than the radius, it might touch the TFCC during wrist movements, a condition known as Ulnar Impaction Syndrome. This may eventually result in TFCC damage.
- Distal Radioulnar Joint (DRUJ) instability: The DRUJ, which connects the radius and ulna, can become unstable, which can put more strain on the TFCC and raise the possibility of injury.
- Sports Injuries: TFCC injuries are more likely to occur in sports like gymnastics that require strong gripping, twisting, or weight bearing on the wrist.
- Occupational Factors: Manual labor, vibration exposure, and repeated wrist movements are some of the occupations that can lead to TFCC injuries.
- Chronic inflammatory diseases, such as gout or rheumatoid arthritis, can impact the TFCC and raise the risk of harm.
- Congenital Factors: People may be more susceptible to TFCC injuries if they have anatomical differences or congenital diseases that alter the structure and stability of the wrist.
Correct diagnosis and management of TFCC damage depend on knowing the underlying etiology. It is advised to speak with a medical expert, usually a hand surgeon or orthopedic specialist, for a precise assessment and suitable treatment.
Symptoms of triangular fibrocartilage complex injuries:
Injuries to the triangular fibrocartilage complex (TFCC) can cause a variety of symptoms, with varying degrees of severity. The following are typical signs of TFCC injuries:
- Wrist Pain: One of the main signs of TFCC damage is wrist pain. The ulnar (pinky) side of the wrist is frequently the site of the pain, which might get worse when you grip, twist, or bear weight.
- Swelling: Swelling around the wrist joint may result from inflammation and fluid buildup within the TFCC.
- Weakness and Instability: TFCC injuries can cause a wrist that feels weak or unstable, which makes it difficult to carry out activities or duties that call for wrist movement.
- Limited Range of Motion: A TFCC injury may be indicated by decreased wrist flexibility and limited wrist mobility, particularly during rotational activities.
- Crepitus: When moving the wrist, especially when twisting it, some people may feel a popping or grinding sound.
- Painful Gripping or Grasping: For those with TFCC injuries, activities involving gripping or grasping items may make wrist pain worse.
- Weight-Bearing Pain: Applying weight to the affected wrist, as in weightlifting or push-ups, might cause pain.
- Painful Wrist Twisting: It can be very unpleasant to twist your wrist, as you might do when opening a jar or turning a doorknob.
- Ulnar Deviation Pain: Lateral wrist movement (toward the pinky side) may cause pain and pain.
- Painful Activities: Typing, playing an instrument, or participating in some sports are examples of activities that require repetitive wrist movements that can worsen pain and discomfort.
- Tenderness: Applying pressure to the ulnar side of the wrist may cause pain since it may be sensitive to the touch.
It’s crucial to remember that the precise kind and extent of the TFCC injury can affect the intensity and mix of symptoms. For an accurate assessment, diagnosis, and suitable treatment, it is best to speak with a healthcare provider if you think you may have a TFCC injury or if you have chronic wrist pain and discomfort.
Pathology of triangular fibrocartilage complex injuries:
Trauma or degeneration can cause a variety of structural alterations and disruptions within the triangular fibrocartilage complex (TFCC), which is part of the pathophysiology of TFCC injuries. The following pathologies are frequently linked to TFCC injuries:
- Tears: The triangular fibrocartilage itself, the ulnar collateral ligament, or the meniscus homolog can all sustain TFCC tears. The wrist’s stability and functionality can be impacted by tears, which can vary in size from minor partial tears to full ruptures.
- Degeneration: The TFCC may experience degenerative changes over time, which might cause its constituent parts to thin, tear, and weaken. Aging, repetitive use, and underlying diseases like arthritis can all hasten degeneration.
- Vascular Changes: Damage to the TFCC might interfere with its blood flow, which hinders its capacity to recover. Delays in recovery and heightened susceptibility to additional harm may result from this.
- Stability: The distal radioulnar joint (DRUJ), which is where the radius and ulna meet, may become unstable as a result of TFCC injuries. Pain, restricted range of motion, and trouble carrying out regular tasks can all be caused by instability.
- Ulnar Impaction Syndrome: This condition, which occurs when the ulna bone strikes the TFCC during wrist movements, can be caused by TFCC injuries. This may result in more deterioration, worse pain, and dysfunction.
- Inflammation: When the TFCC is injured, an inflammatory reaction may be set off, which can cause wrist pain, swelling, and discomfort.
- Secondary Effects: Damage to the TFCC may cause changes in wrist mechanics that impact other joints and structures, such as the ulna, radius, and carpal bones.
- Complications: TFCC injuries can result in reduced wrist function, chronic pain, and the emergence of secondary disorders, such as wrist arthritis, if they are not treated or are not well controlled.
Imaging methods like magnetic resonance imaging (MRI) or arthroscopy are frequently needed to diagnose the precise pathophysiology of a TFCC injury in order to visualize the degree of the damage.
Treatment plans may include conservative methods (rest, splinting, physical therapy) or surgery to repair or reconstruct the TFCC, depending on the severity and kind of the pathology.
For TFCC injuries to be accurately diagnosed and managed, it’s critical to get medical help.
Differential diagnosis:
The symptoms of triangular fibrocartilage complex (TFCC) injuries can be found in a number of diseases. Healthcare providers can choose the best course of action and differentiate between several potential causes of wrist pain with the use of a proper differential diagnosis. When making a differential diagnosis for TFCC injuries, some factors to take into account are:
- Wrist Sprain or Strain: Similar to TFCC injuries, wrist ligament or tendon injuries can cause pain and restricted movement.
- Carpal Tunnel Syndrome: The thumb, index, middle, and ring fingers are frequently affected by this condition, which is characterized by pain, tingling, and numbness in the hand due to compression of the median nerve at the wrist.
- De Quervain’s Tenosynovitis: Pain and restricted movement, particularly during thumb extension and abduction, can be caused by inflammation of the tendons on the thumb side of the wrist.
- Scaphoid Fracture: Often made worse by grasping, a scaphoid fracture can result in wrist pain, soreness, and restricted range of motion.
- Ulnar Collateral Ligament (UCL) Injury: Ulnar side wrist UCL injuries can cause pain and instability, just like TFCC injuries do.
- Ganglion Cyst: A fluid-filled sac called a ganglion cyst may form on the wrist joint, resulting in pain and swelling.
- Kienböck’s disease is characterized by avascular necrosis of the wrist’s lunate bone, which causes pain and restricted wrist motion.
- Rheumatoid arthritis and osteoarthritis are two disorders that can impair wrist function and cause pain and stiffness.
- Intersection Syndrome: Pain close to the wrist joint may result from inflammation of the tendons in the rear of the forearm.
- Radial Tunnel Syndrome: Pain and discomfort in the wrist and back of the forearm may be caused by compression of the radial nerve.
- Tendinitis: Pain and restricted movement may result from inflammation of the wrist tendons.
- Fractures of Other Wrist Bones: Wrist pain and disability may result from fractures of other carpal or metacarpal bones.
- Lunotriquetral Ligament Injury: This ligament can cause instability and pain in the ulnar side of the wrist.
A complete evaluation, including a detailed medical history, physical examination, and frequently imaging tests like MRIs or X-rays, is necessary to properly diagnose a TFCC injury. It’s critical to get medical help if you’re having wrist pain or discomfort in order to receive a proper diagnosis and treatment.
Diagnosis:
Physical Examination:
Patients generally complain of wrist pain on the ulnar side, which frequently worsens with movement. Additionally, there can be clicking, instability, or a weak grasp. There are historical aspects that can coexist with individual sports. Baseball-specific acute injuries, for instance, might result from a hitter becoming “jammed” when attempting to hit an inside pitch or from forceful wrist extension during a head-first slide. Baseball players may sustain chronic injuries as a result of the strain that swinging puts on their wrists. Even if these athletes do not exhibit positive ulnar variance, they may nevertheless have TFCC injuries.
- The ideal way to palpate the TFCC during examination is with the wrist pronated.
- It lies between the os pisiform, ulnar styloid, and flexor carpi ulnaris.
- The diagnosis of TFCC injury may be suggested by a number of physical examination tests.
These include:
- TFCC compression test: symptoms appear when the forearm is in the neutral position with ulnar deviation.
- TFCC stress test: symptoms are produced by applying a force across the ulna with the wrist in ulnar deviation.
- Press test: The press test involves people using their wrists extended to raise themselves off a chair.
- Supination test: The person grasps the underside of a table with their forearms twisted, which limits the TFCC and results in dorsal impingement. If there is a dorsal, peripheral tear, this will produce pain.
- Piano key test: Place your hands on a table for inspection and press your palms against the table. Distal radioulnar joint instability, which may be linked to TFCC injury, is indicated if the distal ulna is prominent on the affected side. This test is considered successful if the palms feel comfortable and the ulnar head rotates to its normal position.
- Grind test: Have the subject twist their forearm while applying pressure to their radius and ulna. A deteriorating process may be indicated by pain.
Evaluation:
A radiograph is usually taken as the first step in the initial workup to check for fractures and measure ulnar variation. An MRI, with or without an arthrogram, is frequently the next step. According to recent evidence, an MR arthrogram is marginally better than an MRI, but considering the additional pain and expense of MRA, it may not be worth doing in place of an MRI. Although CT has a lower sensitivity than MRI, it can be used if MR is not accessible or is not recommended. The most precise method of diagnosing TFCC damage is arthroscopy.
To guide treatment options, it is essential to determine whether the lunotriquetral ligament is damaged or intact. This can be done by searching for a volar tilt of the scaphoid and lunate on a radiograph. Lunotriquetral ligament tears can also be diagnosed by direct sight of the tear or by an arthrogram that shows transmission of contrast.
According to one study, 53% of 85 patients who had surgery to address distal radius fractures also had an arthroscopy-detected TFCC lesion. They did not, however, discover any association between the TFCC lesion and any particular x-ray characteristic. Consequently, TFCC injury cannot be predicted from the first radiograph of a distal radius fracture.
Diagnostic Imaging:
- Radiographs: Avulsion of the ulnar styloid, scaphoid fracture, distal radial fracture, volar tilt of the lunate or triquetrum, and ulnar variance can all be shown on radiographs.
- Triple Injection Arthrography: low specificity tear label.
- MRI: excellent sensitivity and specificity for detecting tears.
Treatment of triangular fibrocartilage complex injuries:
Medical Treatment:
Rest, ice treatment, activity adjustment to remove the cause of the injury, and splint immobilization for three to six weeks should all be part of the rehabilitation program. Physical therapy should also be administered to the patient following immobilization.
- Medication: NSAIDs and other anti-inflammatory drugs can help lower pain and swelling.
- Bracing: Your TFCC can recover if you use a brace or splint to keep your wrist and forearm stable.
- Injections: Cortisone injections aid in minimizing tissue tearing and swelling.
Surgical Treatment:
In the event that conventional treatment is ineffective or there is distal radioulnar joint instability, surgical options should be explored. The Palmer classification of the injury will determine the course of surgical treatment.
The most well-known scheme for TFCC lesions is the Palmer classification, which divides them into these two groups (with other subcategories that are outside the purview of this article):
- Traumatic and Degenerative: Although it provides a precise anatomical explanation for the tear, this categorization is not used to guide treatment or predict prognosis.
- A debridement is a surgical procedure that induces bleeding in order to promote healing. Debridement is beneficial for central TFCC tears, although it has been demonstrated to have more dangerous effects on patients with larger positive ulnar variation or degenerative tears.
Physical Therapy Treatment:
- Corticosteroid injections, physical therapy, and rest are the main forms of treatment.
- There are differences in how long one should try conservative treatment before considering surgery.
- If there is no distal radioulnar joint (DRUJ) instability, conservative treatment for six months is appropriate.
Post-Operative Rehabilitation:
Although recovery from surgery varies, an open approach should take around three months, and an arthroscopy should take four to six weeks. Physical rehabilitation will be administered to patients following the surgery. The type of surgery done and the surgeon’s preferences determine when physical therapy should begin and how long it should last.
For type 1 injuries:
- Following the arthroscopy, the wrist will be immobilized for a week.
- Range-of-motion exercises can be started after a week.
- Three weeks following the arthroscopy, golfers and tennis players who suffer from a stable TFCC tear can start modest exercise, ball contact.
- In four to six weeks, they might resume their regular sporting activities. An ulnocarpal corticosteroid injection can be a possibility if the symptoms persist.
- Post-operative immobilization in a Muenster cast for four weeks may be suggested for more severe damage.
Basic range of motion exercise:
Please be aware that these are merely introductory exercises and should only be carried out with a trained healthcare provider’s supervision. Triangular fibrocartilage complex (TFCC) injuries may benefit from the following range-of-motion exercises:
- Wrist Flexion: Bring the palm to the forearm by slowly bending the wrist forward. Hold for a few seconds, then let go.
- Wrist Extension: Point the fingers toward the ceiling while slowly bending the wrist backward. Hold on for a moment, then let go.
- Wrist Supination: As though you were carrying a bowl of soup, turn your forearm and palm upward.
- Wrist Pronation: As though you were pouring down a cup of soup, rotate your forearm and palm downward.
- Ulnar Deviation: Tilt your hand and wrist slowly in the direction of your pinky.
- Radial Deviation: Tilt the hand and wrist slowly in the direction of the thumb.
Passive Range of Motion (PROM) Exercises:
Gently move the damaged wrist through its range of motion with a different hand, being cautious not to push through any painful activities. Understand that these workouts shouldn’t make symptoms worse and should be done in a pain-free range. If someone’s pain or discomfort improves, cease the exercises and speak with their doctor. A physical therapist can help you follow an exercise regimen designed to meet your unique TFCC injury and recovery requirements.
After 4 weeks:
- The wrist is placed in a Versa wrist splint or short arm splint, which allows for progressive wrist motion.
- Immobilization will reduce wrist pain and discomfort, which may promote healing.
- The wrist will become more stable with the use of certain types of splints, improving hand function.
- After that, patients can start with grip-strengthening and range-of-motion activities.
- Because eccentric grip-strengthening exercises affect the co-activation pattern of the wrist flexors, which aid in wrist stabilization, therapists are more likely to recommend them.
- To increase overall wrist stability, further co-activation exercises could be added.
- When using a VersaSplit, a device for wrist and hand rehabilitation, wrist exercises should be performed carefully and ideally with a healthcare provider’s supervision.
- A few possible exercises are as follows:
Wrist Flexion and Extension (With VersaSplit):
- In the VersaSplit, secure the wrist.
- Move the palm toward the forearm to perform controlled wrist flexion.
- Move your fingers toward the ceiling to perform controlled wrist extension.
- To achieve a comfortable range of motion, repeat these steps.
Wrist Radial and Ulnar Deviation (With VersaSplit):
- Keep your wrist in the VersaSplit securely.
- Tilt the hand and wrist gently in the direction of the pinky side (ulnar deviation).
- Tilt the hand and wrist gently in the direction of the thumb (radial deviation).
- Perform these movements in a range that feels comfortable.
Grip Strengthening (With VersaSplit):
- Use the VersaSplit’s resistance to work on grip-strengthening activities.
- Release the device after a few seconds of holding it against resistance.
- Continue for the predetermined number of times.
Wrist Circles (With VersaSplit):
- Make gradual clockwise and counterclockwise wrist circles while the wrist is securely fastened in the VersaSplit.
- Focus on keeping your movements fluid and under control.
Pronation and Supination (With VersaSplit):
- In the VersaSplit, secure the forearm.
- Supination is the upward rotation of the forearm and palm.
- Rotate your palm and forearm downward, or pronate.
Always prioritize your health and safety when performing these activities. As you become more comfortable, progressively raise the resistance from low. Stop the exercises and speak with your doctor or physical therapist if you feel pain, discomfort, or if your symptoms get worse. Depending on your demands and condition, they might offer appropriate advice.
At 8 weeks post-operative:
- It is time to begin active muscle training.
- It is advised to follow a progressive pain-free workout regimen.
Activity modification and patient education are essential components of physical therapy treatment. To help strengthen the area and lower the risk of instability, isometric exercises should be used. Isometric exercises are appropriate for wrist and finger rehabilitation in situations with triangular fibrocartilage complex (TFCC) injuries because they can assist in strengthening muscles without generating joint movement. Keep in mind that these exercises should be done slowly and painlessly.
Wrist Flexion Isometric Exercise:
- Place the palm of the forearm facing up on a surface.
- Cover the damaged hand with your other hand.
- Without allowing any movement, push the damaged hand upward against the opposing hand’s resistance.
- Hold for 5–10 seconds, then let go. Do this a couple of times.
Wrist Extension Isometric Exercise:
- With the palm facing down, place the forearm on a surface.
- Cover the damaged hand with your other hand.
- Without allowing any movement, press the injured hand downward against the opposing hand’s resistance.
- Hold for 5–10 seconds, then let go. Do this a couple of times.
Finger Isometric Exercise (Grip):
- Make use of a stress ball or a softball.
- Squeeze the ball slowly with your fingers, then hold the contraction for five to ten seconds.
- Relax and let go of the hold. Repeat a number of times.
Finger Isometric Exercise (Spread):
- Place the hand flat, fingers slightly apart, on a surface.
- Without allowing your fingers to move, create resistance by pressing them outward against the surface.
- After 5–10 seconds, let go and unwind. Do this a couple of times.
- Try to stay away from any activity that makes you feel uncomfortable or in pain, and always pay attention to your body. Start with a modest resistance and gradually increase it as your strength grows.
- Seek advice from a medical expert or physical therapist who can prescribe the best workouts for your TFCC injury if you’re unsure or in pain. Unilateral isometric exercises are beneficial in particular since they have been shown to enhance bilateral voluntary muscle activation.
- This might be the outcome of increased neuromuscular control caused by stimulation of the motor cortex.
- Furthermore, the pronator quadratus controlled isometric activation in neutral wrist posture and supination will aid in stabilizing the distal radioulnar joint (DRUJ).
- In patients with TFCC injuries, this can be used both before and after surgery.
At three months:
People are likely to resume their regular activities after surgery.
A further three to four months are needed to resume regular sporting activity.
Passive Mobilisation:
The first way to find out if this causes pain is to flex the midcarpal and radiocarpal joints. A dorsal sliding technique can be applied to encourage wrist flexion. Techniques for passive mobilization can help with problems like limited wrist flexion and increase wrist flexibility. This is an explanation of the “dorsal sliding” passive mobilization method for wrist flexion:
Passive Mobilization –Wrist Flexion Dorsal Sliding:
- By providing controlled pressure to the dorsal (rear) side of the wrist, this treatment seeks to improve joint mobility and promote sliding of the carpal bones while gradually increasing wrist flexion.
- The recipient of the mobilization should be lying down or sitting comfortably.
- The mobilizer, who is usually a licensed medical practitioner or physical therapist, should arrange themselves such that they can easily reach the wrist.
- With one hand supporting the forearm and the other gently cradling the back of the wrist joint, the mobilizer places their hands on the dorsal side of the wrist.
- In order to encourage the carpal bones to slide and the wrist joint to shift into flexion, the mobilizer gently and steadily applies posterior (rearward) pressure on the wrist.
- The mobilization should be carried out with regulated pressure and within a pain-free range of motion.
- To guarantee comfort and prevent using too much power, the mobilizer keeps in touch with the person getting the treatment.
- Usually, the mobilization is held for five to ten seconds before being released.
- A few repeats of this procedure might be made, progressively increasing within the person’s tolerance.
- It is crucial that the person receiving the method and the mobilizer communicate openly. Feedback regarding their degree of comfort and any feelings they may have should be given by the individual.
Post-Mobilization Stretching:
It is possible to increase flexibility by adding a little wrist flexor stretching after the mobilization. This can be accomplished by applying a controlled stretch to the wrist’s palm side using the other hand.
The volar sliding technique can be used to promote wrist extension. Indeed, this is a summary of the “volar sliding” passive mobilization approach for wrist extension. By providing controlled pressure to the volar (palm) side of the wrist, this approach seeks to improve joint mobility and promote the sliding of the carpal bones, so gradually increasing wrist extension.
Passive Mobilization – Wrist Extension Volar Sliding:
- In order to induce the carpal bones to slide and the wrist joint to go into extension, this treatment applies regulated anterior (forward) pressure on the palm side of the wrist.
- The recipient of the mobilization should be lying down or sitting comfortably.
- The mobilizer, who should ideally be a licensed medical practitioner or physical therapist, should arrange themselves such that they can easily reach the wrist.
- With one hand supporting the forearm and the other gently cupping the palm side of the wrist joint, the mobilizer places their hands on the volar side of the wrist.
- To encourage the carpal bones to slide and the wrist joint to move into extension, the mobilizer exerts anterior (forward) pressure on the wrist gradually and softly.
- The mobilization should be carried out with regulated pressure and within a pain-free range of motion.
- To guarantee comfort and prevent using too much power, the mobilizer keeps in touch with the person getting the treatment.
- Usually, the mobilization is held for five to ten seconds before being released.
- Work slowly inside the person’s comfort zone as you repeat the method a few times.
- Keep lines of communication open between the person receiving the technique and the mobilizer.
- Feedback regarding their degree of comfort and any feelings they may have should be given by the individual.
Post-Mobilization Stretching:
Following the mobilization, think about adding a little wrist extensor stretch using the opposing hand to give the dorsal side of the wrist a controlled stretch.
As with any passive mobilization method, it’s crucial to make sure a trained practitioner with manual therapy experience performs it. See a doctor or physical therapist if you’re having wrist problems or are thinking about using such treatments. They can assess your condition and offer the right advice and care.
The ulnar sliding technique may be applied to aid with the radial deviation.
The radial sliding technique may be applied to aid with the ulnar deviation.
Indeed, passive mobilization strategies for both radial and ulnar wrist abnormalities are described here.
By applying regulated pressure to the wrist, these procedures seek to improve joint mobility and promote the carpal bones’ sliding in certain directions, thereby gradually increasing range of motion.
Passive Mobilization – Ulnar Sliding for Ulnar Deviation:
- In order to induce the carpal bones to slide and the wrist joint to migrate into ulnar deviation, this treatment applies controlled pressure on the ulnar side of the wrist.
- The recipient of the mobilization should be lying down or sitting comfortably.
- The mobilizer, who should ideally be a licensed medical practitioner or physical therapist, should arrange themselves such that they can easily reach the wrist.
- With one hand supporting the forearm and the other gently cupping the ulnar side of the wrist joint, the mobilizer places their hands on the wrist’s ulnar side.
- In order to encourage the carpal bones to slide and the wrist joint to shift into ulnar deviation, the mobilizer gently and steadily applies lateral (sideways) pressure to the wrist.
- The mobilization should be carried out with regulated pressure and within a pain-free range of motion.
- To guarantee comfort and prevent using too much power, the mobilizer keeps in touch with the person getting the treatment.
- Usually, the mobilization is held for five to ten seconds before being released.
- Work slowly inside the person’s comfort zone as you repeat the method a few times.
Passive Mobilization – Radial Sliding for Radial Deviation:
- In order to induce the carpal bones to slide and the wrist joint to shift into radial deviation, this treatment applies controlled pressure on the wrist’s radial side.
- The same preparation procedures should be followed for the ulnar sliding technique.
- With one hand supporting the forearm and the other gently cupping the radial side of the wrist joint, the mobilizer places their hands on the wrist’s radial side.
- To encourage the carpal bones to slide and the wrist joint to shift into radial deviation, the mobilizer delivers lateral (sideways) pressure on the wrist gradually and softly.
- Make that the mobilization is carried out with regulated pressure and within a pain-free range of motion. To guarantee comfort and safety, communication with the individual receiving the method is essential.
- Usually, the mobilization is held for five to ten seconds before being released.
- Work slowly inside the person’s comfort zone as you repeat the method a few times.
- As with any passive mobilization method, it’s crucial to make sure a trained practitioner with manual therapy experience performs it. See a doctor or physical therapist if you’re having wrist problems or are thinking about using such treatments. They can assess your condition and offer the right advice and care.
General Mobility Exercises:
Wrist rotations:
- Depending on the variant one chooses, wrist rotations are a simple exercise to master and require little to no equipment to perform.
- The arms should be straight out in front of you to begin.
- Make a fist with your hands and begin turning your wrists outward in a circle.
- begins slowly in a small circle and gradually increases the range of motion as you proceed.
- Rotate in a different direction after repeating for 10 to 15 seconds.
Horizontal ulnar and radial deviation:
- In order to produce the radius and ulna parallel, start by sitting next to the table with the affected arm, if at all possible, flexed at 90 degrees. Place the involved hand palm down on the picture receptor with the hand in radial deviation, shoulder, elbow, and wrist all in the transverse plane, vertical to the central beam. This shortens the radius relative to the ulna.
Active pronation and supination:
- Begin by keeping the arm that needs to be worked out resting on a table while sitting upright.
- Hold a pen or spoon in your hand, with the thumb side of your hand receiving the majority of the spoon’s length.
Wrist Flexion Stretch:

- Press the hand’s return and keep it down for 15 to 30 seconds with the other hand to assist in flexing the damaged wrist downward.
- After that, push the fingers backward and hold the hand for 10 to 20 seconds to extend it back.
- Perform five sets.
Wrist Extension Stretch:
- To begin, stand at a table with your elbows straight, your palms down, and your fingers flat.
- The weight should be leaned forward.
- Hold this posture for fifteen seconds.
- Do this three times.
Wrist Extension With Dumbbell:
- A chair, a table or desk, and a dumbbell are required for the wrist extension.
- To begin, place your forearm on a table while seated in a chair.
- Hang your hand and wrist over the side of the table while holding a 2- or 3-pound dumbbell.
- Lift the hand slowly such that the back pushes toward the ceiling while the palm is facing down.
- Keep your forearm on the table.
- Hold the position for a few seconds when the wrist is fully extended, and then slowly bring your hand down.
- Ten to fifteen times, repeat this motion. Do two or three sets.
Dumbbell Wrist Flexion:
- Put the forearm back on the table and continue to support the weight. With the palm facing the ceiling, turn the hand over.
- Keep your arm back against the table.
- The palm should then push toward the ceiling as you flex your wrist.
- Hold the wrist in this posture for two to three seconds after it is fully flexed.
- After that, slowly return the hand to its initial position.
- For two to three sets of ten to fifteen repetitions, repeat the wrist flexion action.
- You can also perform this exercise without a dumbbell.
Prayer Stretch:
- Begin with a posture as though in prayer, stand with your elbows bent, and place your palms together, fingertips up, slightly below your chin.
- Drop the fingers while keeping them together until the insides of your arms start to stretch.
- Keep the fingers together, but let the palms be apart.
- Hold for 30 seconds.
Steeple Stretch:
- Start this stretch from above in the “prayer” stance.
- Spread the thumbs and fingers as widely as is comfortable.
- Separate the palms while holding the fingers together, then reunite them.
- Do a few reps several times a day.
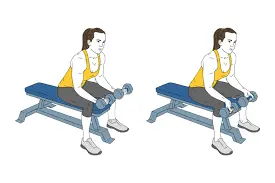
Wrist Supination With Dumbbell:
- To begin, place your wrist and hand over the edge of a chair while the side of your forearm rests on the table. The ceiling should be the thumb’s orientation.
- Hold the end of a small dumbbell that weighs between one and three pounds in the same manner as you would a hammer.
- Allow the hand and wrist to slowly turn such that the palm is facing the ceiling.
- After a few seconds of holding the hand in the stop position, slowly twist it back up until the dumbbell is straight up again.
- One can alternate between rotating their wrist in the supination and pronation movements described in the following step.
Wrist Pronation With Dumbbell:
- The attitude of the hand facing down, as though pouring water from a pitcher, is driven by wrist pronation.
- Sit in a chair with your wrist and hand over the edge and your forearm resting on a table to strengthen your wrist pronators.
- With the weight pointing upward toward the roof, hold one end of a dumbbell.
- Rotate the hand slowly until the palm and wrist are pointing downward toward the ground.
- After a few seconds of holding this posture, slowly rotate the hand back to the initial position, this time with the weight pointed upward toward the ceiling.
- Do 10–15 repetitions of this exercise in two or three sets.
- Turn the palm up and down alternately if you combine this action with wrist supination (in the previous step).
Prevention:
Not every accident that tears your TFCC can be avoided. However, you can reduce your risk of a TFCC tear by doing the following:
- Before participating in a sport or activity that requires wrist or arm twisting, such as baseball or tennis, warm up with some exercises.
- Build up your forearm and wrist muscles.
- To avoid falls, pay attention to your footing as you’re walking.
Complications:
The majority of complications are associated with surgical management. Infections, hypertrophic scarring, tendon damage, nerve damage, reflex sympathetic dystrophy, and stiff joints with restricted range of motion are a few examples of postoperative problems.
Prognosis:
In general, the prognosis for TFCC injury is good. When combined with ulnar shortening osteotomy, arthroscopic repair and arthroscopic debridement have both been demonstrated to be successful procedures. Because surgical therapy has been shown to have positive results in pediatric and teenage high-level athletes who wish to resume sports, it also has a promising prognosis for children.
After arthroscopic debridement, 70% of 71 patients under 45 with a central TFCC tear were satisfied, according to one study. Additionally, they discovered that worse results were typically associated with degenerative tears and larger positive ulnar variance. A negative DRUJ stress test, being a woman, and having symptoms for a prolonged period are some bad prognostic markers. Patients who follow postoperative recommendations have the best long-term prognosis.
Even while physical therapy or surgery can help most people recover completely from a TFCC rupture, you can experience moderate wrist pain or stiffness for years after the injury. To treat any an ongoing pain or stiffness, consult with your physician. You might need to continue physical therapy or wear a brace while performing specific tasks, depending on how much pain you are experiencing.
With rest and rehabilitation, the majority of mild TFCC tear can heal on their own. More serious tears can be repaired surgically. After surgery, the majority of patients with TFCC tears return to full function in 12 weeks.
Conclusion:
Your wrist may become painful and unstable due to tears in the triangular fibrocartilage complex (TFCC). A TFCC rupture can frequently be healed with straightforward therapies like physical therapy and rest. More severe tears may require surgery to mend. Most patients with TFCC tears recover full function in a few months with the correct care.
FAQs
How does one go about fixing a TFCC?
Both open and arthroscopic techniques can be used to repair TFCC lesions. Arthroscopic TFCC repair: This less invasive method involves making two to three incisions in the wrist, each around 5 mm in size. An arthroscopic telescope and other surgical tools are then introduced into these incisions.
Will a TFCC tear be shown on an MRI?
Ulnar-sided wrist pain is often caused by injuries to the TFCC. With the right technique and interpretation, MRI offers excellent characterization of TFCC tear and the wrist disease associated with them. It also enables reliable pre-treatment evaluation of patients with suspected TFCC pathology.
How much time does it take for an injury caused by the TFCC to heal?
Depending on whether surgery is required, recovery times for TFCC (Triangular Fibrocartilage Complex) injuries might vary. Non-surgical patients usually take 4-6 weeks, whereas surgical cases may take 6 weeks to several months to fully recover.
Which is better for TFCC, heat or ice?
Reducing pain and inflammation in the surrounding area is the first goal of treatment for a TFCC injury at Fast Track Physical Therapy. Just applying ice to your wrist helps reduce inflammation and frequently alleviates a significant amount of pain. Heat may be more beneficial in situations involving more persistent pain.
What proportion of TFCC tears need to be surgically repaired?
Additionally, these symptoms were signs that surgery was necessary. The number of patients who had open procedures following unsuccessful conservative measures was recorded in two trials. Overall, following conservative measures, 44% (52/119) of patients with TFCC injuries had surgery.
How might TFCC recovery be accelerated?
While the tear heals, the first step in treating TFCC tears is to temporarily cease engaging in any activities that produce wrist pain. To keep your wrist from moving, you might need to wear a cast or splint. Your physician will probably suggest physical treatment for roughly six weeks.
Which exercises are best avoided when using TFCC?
keep away of pectoralis (chest) strengthening exercises, push-ups, pull-ups, pull-downs with the wrist supinated, and bicep curls. You must stretch these muscles These muscles need to be lengthened, yet strengthening them has the opposite effect.
Can an x-ray show a TFCC tear?
When examined by a radiologist, tears or damage to the TFCC should be apparent; nevertheless, occasionally nothing unusual is observed.
Can surgery be used to heal TFCC?
Can a Tear in the TFCC Heal Without Surgery? Yes, a TFCC tear can mend without surgery, is the short answer to this query. It’s crucial to realize that without surgery, the area toward the outside of the wrist will recover more quickly, and that your pain may not go away right away.
What occurs if treatment for a TFCC tear is not received?
A tear might throw off the balance of the TFCC, which is essential for wrist stability. If left untreated, TFCC tear can cause weakness, chronic pain, and restricted motion, which makes daily tasks more difficult.
Does a TFCC tear appear on an MRI?
Conventional MRI scan Conventional MRI can identify a TFCC tear with high throughput. The sensitivity, specificity, and accuracy were 92%, 89%, and 91%, respectively, according to a recent study by Zlatkin et al.
Are TFCC shirts proper for doing weights?
The suggested procedures during primary inflammation are immobilization, ice, and rest (no lifting, activity, or movement). For a wrist injury, the ideal position is supported and neutral (see left).
How dangerous is a TFCC tear?
Surgery may be necessary in certain instances of severe TFCC damage. A hand ligament injury frequently necessitates surgery. Your doctor might recommend physical therapy for a few weeks following surgery and recovery to help your wrist regain its range of motion and flexibility.
Are TFCC injuries self-healing?
The kind, nature, and severity of the injury determine the available treatment options for TFCC tears. A TFCC rip will mend itself in certain circumstances. To stop additional damage and give the affected wrist time to heal, one should avoid from using it.
What is the duration of the triangular fibrocartilage complex’s healing process?
Four to six weeks are often needed for recovery from TFCC injuries that don’t require surgery. It could take six weeks to many months to fully regain wrist function if surgery is required. You can speed up your recovery with physical therapy and by avoiding wrist-pressure-causing activities.
References
- Thakkar, D. (2023, August 29). Triangular fibrocartilage Complex injury – Samarpan. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/triangular-fibrocartilage-complex-injury/
- Triangular Fibrocartilage Complex TeAR (TFCC). (2025, March 19). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/21832-triangular-fibrocartilage-complex-tear-tfcc
- Casadei, K., & Kiel, J. (2023, August 14). Triangular fibrocartilage complex. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537055/
- Adcox, M. (2018, September 18). Understanding TFCC tears. Healthline. https://www.healthline.com/health/tfcc-tear