Subscapularis Muscle Pain
What is a Subscapularis Muscle Pain?
Subscapularis muscle pain can significantly impair shoulder function and quality of life. As one of the key muscles comprising the rotator cuff, the subscapularis plays a vital role in stabilizing and facilitating shoulder movements. However, various factors such as overuse, injury, poor posture, or muscle imbalances can lead to pain and dysfunction in this muscle.
Anatomy of Subscapularis Muscle
Originating from the subscapular fossa, the subscapularis muscle is a large, triangular muscle. “Subscapularis” translates to “under (sub) the scapula,” or wing bone.
It is one of the rotator cuff’s four muscles; the other three are the teres minor, infraspinatus, and supraspinatus. The longest and strongest rotator cuff muscle is the subscapularis.
Origin
the subscapular fossa’s medial two-thirds.
Insertion
The fibers form a tendon that enters into the front of the shoulder joint capsule and the lesser tubercle of the humerus.
Nerve Supply
The posterior chord of the brachial plexus stimulates the C5–C6 upper and lower subscapular nerves.
Both the upper and lower subscapular nerves, which originate from the posterior chord of the brachial plexus, stimulate the subscapularis.
While the lower subscapular nerve splits into two, with one branch providing the lower part of the subscapularis, the upper subscapular nerve serves the upper section of the subscapularis.
Blood Supply
Subscapular artery
Action
The humerus’s internal rotation serves as the initial function. In some postures, it helps with shoulder adduction and extension.
The subscapularis muscle acts differently depending on the position of the arm. For example, when the arm is raised, it pulls the arm forward and downward. Similarly, when the humerus is fixed, the insertion of the subscapularis muscle may act as an origin and cause the inferior border of the scapula to abduct.
The Subscapularis, a component of the rotator cuff, is essential for shoulder stabilization.
Causes of Subscapularis Muscle Pain
Overuse or tension on a muscle is a common cause. The following are some specific reasons for this particular muscle:
- Reaching back to break- a fall—sudden overload
- Any damage or displacement to the shoulder joint
- extended shoulder immobilization in an adducted and medially rotated posture
- Overhead lifting that is excessive
- internal rotation repetitive motion (throwing a ball, swimming)
- forward-leaning head position that causes the shoulder to rotate inward too much
Pathologies
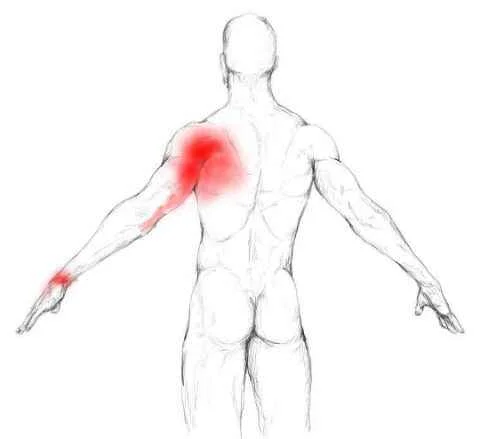
- Up to three trigger sites can be found in the subscapularis, the two most common of which are located close to the muscle’s outer border.
- Fortunately, there isn’t much of a trigger point on the inside border of the muscle because it’s practically hard to palpate and manually release.
- Trigger points in the subscapularis muscle refer pain mostly to the posterior shoulder, with a surplus extending into the area between the shoulder blades and along the back of the upper arm.
- Most people are aware of this wrist discomfort, but they do not believe it is connected to their shoulder ache.
- Throwers often cause injuries to it.
- Pain and soreness will result from applying pressure to the tendon’s insertion, which is located inside the upper arm.
- Symptoms of subscapularis tendinitis include soreness in the shoulder when moving, especially when the arm is elevated above the shoulders.
- Overuse of the subscapularis muscle might give the impression that one is unable to raise one’s arm. It might even be the cause of a frozen shoulder.
Symptoms of Subscapularis Muscle Pain
- Shoulder pain, most especially at the front of the shoulder, is the most common sign of a subscapularis rupture.
- When rotating their arm, a person may also experience or hear a “clicking” sound in their shoulder.
- There are certain signs of other rotator cuff tears that are quite similar to those of a subscapularis tear. discomfort that worsens at night
- weakness in the arms or shoulders
- Pain that worsens when one raises their arm
- Other subscapularis tear symptoms are peculiar to this type of injury. These comprise:
- weakness in the biceps
- Finding it difficult to reach for the rear of something or the back pocket
- discomfort beneath the collarbone
- With its palm facing forward, the wounded arm rotates outward without the person moving it.
Diagnosis
The doctor will first take a thorough medical history. They’ll inquire about any recent injuries you may have had to your arm or shoulder, your specific symptoms, and any tasks you’re finding difficult.
After that, tests will be performed to help identify potential causes of your pain. Your doctor may perform several tests to aid in the diagnosis of a subscapularis tear. Among them are the following Special test
Special test
Lift-Off Evaluation test
The lift-off test, often known as “Gerber’s Test,” was first described by Gerber and Russell in 1991.
- The patient is instructed to place their hand behind their back, with the dorsum resting on the area of the mid-lumbar spine, while they are being evaluated standing up.
- By preserving or strengthening the internal rotation of the humerus and extension at the shoulder, the dorsum of the hand is elevated off the back.
- A typical lift-off test consists of the ability to actively elevate the hand’s dorsum off the back.
- The inability to move the dorsum of the back suggests a dysfunctional or aberrant lift-off test and a ruptured subscapularis.
Bear Hug Test
The Bear Hug Test involves the subject placing the palm of their injured arm on their non-affected shoulder while in the maximum anterior translation posture with their elbow in front of their torso.
The doctor applies an externally rotating force on the patient’s forearm, instructing them to hold their initial posture.
If the patient is unable to hold the position of his arm or exhibits weakness in internal rotation when compared to the opposite side, this suggests a tear or dysfunction in the subscapularis muscle. The test is considered positive.
Belly Press Test
The afflicted arm is held at the side, the shoulder flexed to a 90-degree angle, and the palm of the hand rests on the subject’s abdomen to perform the Belly Press Test.
A person is told to perform an internal rotation by pressing the palm of his hand on his abdomen.
If the subject exhibited weakness in internal rotation in comparison to the other side, or if the internal rotation was not felt when pressing on his belly, but rather shoulder extension or elbow, the test was considered successful.
Differential diagnosis
The differential diagnosis is broad and includes
- septic shoulder
- myonecrosis
- calcific tendinitis
- polymyositis
- muscle strain
- intramuscular hematoma
- acute osteomyelitis
- sarcoma.
It is based only on the history and clinical findings.
Treatment of Subscapularis Muscle Pain
Conservative treatment for tendinopathy and subscapularis pain involves rest, ice, analgesics, activity modification, and physical therapy. Ice therapy mainly reduces pain and inflammation.
When using the thumb technique to massage the subscapularis muscle, feel the muscle contract. Then, release the tension and start stroking the area.
Make sure the individual is massaging the muscle, not the surrounding tissue.
If not, the person may experience pain for several days as a result of stressing the nerves in the armpit rather than the muscle.
Depending on how bad the inflammation can get, there may be several approaches to treating subscapularis tendinitis.
Anti-inflammatory drugs and hot or cold therapy can be used to treat a mildly or moderately inflamed subscapular tendon.
In order to assist stop the disease from getting worse, it will be advised that the patient rests for at least one to two weeks during the course of treatment.
The subscapularis tendon is an essential component of the rotator cuff and shoulder joint, hence one should exercise caution when handling it.
Surgical treatment is required for a tear that is accompanied by tendon inflammation, and this involves exposing the tendon in order to identify the damaged ligament.
The physician will next separate and remove the rotator cuff’s damaged tendon and restore the nearby normal tendon to its original location.
Physiotherapy treatment of Subscapularis Muscle Pain
Physiotherapy can be an effective treatment approach for subscapularis muscle pain. A physiotherapist can assess your condition, identify contributing factors, and develop a customized treatment plan to address your specific needs. Here are some common physiotherapy treatments for subscapularis muscle pain:
- Manual Therapy: Hands-on techniques such as massage, soft tissue mobilization, and joint mobilization can help reduce muscle tension, improve flexibility, and restore normal joint mechanics.
- Stretching Exercises: Gentle stretching exercises targeting the subscapularis and surrounding muscles can help alleviate tightness, improve flexibility, and reduce pain. Your physiotherapist can teach you specific stretches tailored to your condition.
- Strengthening Exercises: Strengthening exercises are crucial for restoring muscle balance and stability around the shoulder joint. Your physiotherapist may prescribe exercises to strengthen the subscapularis, as well as other muscles involved in shoulder movement and stability.
- Postural Correction: Addressing postural issues is essential for preventing further strain on the subscapularis muscle. Your physiotherapist can provide guidance on proper posture during daily activities and recommend exercises to improve posture.
- Modalities: Modalities such as heat therapy, cold therapy, ultrasound, or electrical stimulation may be used to reduce pain, inflammation, and muscle spasms.
- Activity Modification: Your physiotherapist may advise you to modify or avoid activities that exacerbate your symptoms, especially those involving repetitive overhead movements or heavy lifting.
- Education and Self-Management: Understanding your condition and learning self-management strategies are essential for long-term recovery. Your physiotherapist can educate you on proper body mechanics, ergonomic principles, and home exercises to maintain progress and prevent recurrence of symptoms.
- Progressive Rehabilitation: As your pain improves and your shoulder function restores, your physiotherapist will gradually progress your rehabilitation program to challenge your muscles and improve overall function.
It’s important to follow your physiotherapist’s recommendations and adhere to your treatment plan consistently for optimal results.
Exercises for Subscapularis Muscle
Following subscapularis muscle soreness, the patient will go through five phases that gradually restore shoulder strength and range of motion.
The five phases are:
- the time of maximum protection with only passive mobility.
- the first phase of muscle endurance with active exercise.
- the stage of resistance training that builds muscle strength.
- strengthened muscles and a return to regular activities.
- a return to regular athletic competition.
Phase 3 has been reached by one person. They can do these exercises every day at home:
Stretches of subscapularis muscle
- Towel extension stretch
- Finger walk
- Cross-body St-reach Sit and stand
- Armpit stretch
- Outward rotation
- Inward rotation
- Bent-arm Wall Stretch
- Bent Arm Scaption Plane Stretch
- Extended Child’s Pose on Fingertips
Towel extension stretch
- With one hand, hold the three-foot-long towel behind your back, and with the other, grip the opposite end.
- It is held horizontally with the towel.
- An advanced variant of the exercise is also carried out, where the towel is draped over the good shoulder.
- Holding the towel’s bottom in the afflicted arm, move the unaffected arm’s hand towards the lower back.
- You perform ten to twenty repetitions of this exercise every day.
Finger Walk on Finger ladder
- At three-quarters of arm’s length, face the wall.
- With the affected arm extended, reach out and make contact with the wall at waist level.
- Move your fingers like a spider and travel gently up the wall with your elbow slightly bent until your elevated arm is as high as it gets. the finger alone—the shoulder muscles are not involved.
- Repeat, moving slowly down the lower arm.
- Ten to twenty times a day, perform this workout.
Cross-body stretch
Gently apply pressure to the affected shoulder to extend it by lifting the affected arm at the elbow and moving it up and across the body with the unaffected arm.
Stretch your armpit
- Raise the afflicted arm to about breast height using the strong arm.
- Open up the armpit and gently bend the knees.
- Bend your knees somewhat deeper and softly extend your armpit.
- Bend and stretch a little bit more with each knee, without pushing yourself.
Rotation outward
- With your elbows bent 90 degrees towards the sides, grab the rubber exercise band in the space between your hands.
- Rotate the affected arm’s bottom portion outward by two or three inches, then hold the position for five seconds.
- Once a day, perform this exercise ten to fifteen times.
Rotation inward
Place one end of the rubber exercise band around the doorknob while standing next to the closed door.
Hold the elbow at a ninety-degree angle while grabbing the opposite end in the hand of the injured arm.
After pulling the band two or three inches towards the body, hold it there for five seconds.
Once a day, perform this exercise ten to fifteen times.
Wall Stretch with the Bent Arm
The individual receiving care takes on a split stance where you are in a doorway and at the end of a wall with your right leg in front and your left leg behind.
Next, Raise the left arm to shoulder level and place the inside of the arm and palm on the wall or doorway.
The arm of the sufferer resembles a goalpost.
Next, to feel the stretch, gently press your chest through the opening.
Stretching the different parts of the chest is possible by raising and lowering the arm.
Then carry out the same exercise on the opposite side.
Scaption Plane Stretch with Bent Arm
You are kneeling in front of a raised object.
Next, place one palm on the surface, extending the elbow joint. Make an effort to roll the shoulder capsule in and out.
This stretching stance gives you the greatest stretch in your pec.
After that, perform 10 ins and outs of the stretch, holding each pose for 15 to 30 seconds.
Perform the 3 reps in 1 set three times a day.
Pose of an Extended Child on Fingertips
The sufferer is on their knees on the ground.
When the patient is sitting on their heels, try to touch their big toes together.
Next, divide the knee joint to a width equal to that of the hip joint.
Next, extend the hands as far in front of them as you can while bending forward from the hip joint.
Arms outstretched, palms down, then rise up onto fingertips as though the ball beneath the
Exercises
- Pendulum
- Passive Internal Rotation
- Internal Turning
- Horizontal Abduction Prone
- Scapular Stabilization Exercises
- Shoulder joint internal rotation isometric exercise
- Chin-ups
- Lateral raises
- Internal rotation with abduction
- Reverse Lawn mower starter
- Shoulder blade squeeze
- Shoulder raises
- Shoulder rolls
- Wide-legged standing forward bend
- T, Y & I movements
- Cow face pose
- Eagle arms spinal rolls
- Cross-body arm swings
Pendulum
One can ease themselves into shoulder rotation with this practice.
- Step 1: Lean forward, place one hand on a counter or tabletop for support, and free the other hand.
- Step 2: Swing the arm slowly side to side, back and forth. Carry out the same action using the opposite arm.
- Do these steps twice a day for ten repetitions.
Passive Internal Rotation
This is an excellent exercise to increase the range of motion and stretch the subscapularis.
- Step 1: Reach behind your back for a stick, yardstick, or light pole. With your other hand, slowly hold onto the other end of the stick.
- Step 2: draw the stick in a horizontal direction to draw the shoulder passively. It should pull on a person, but not hurt. For thirty seconds, hold.
Internal Rotation
This is an active workout that uses a resistance band. Shoulder muscles will become stronger with this exercise.
- Step 1: Attach a resistance band at hip length to a doorknob or table leg.
- Step 2: Bend your elbow to the side and grab the band. Bring the arm across the torso while maintaining a close elbow stance.
- Step 3: Repeat after carefully putting the arm back in its initial position.
- Do the same on the other side. Do eight repetitions on each side for three sets.
Horizontal Abduction Prone
The primary goal of this exercise is to improve subscapular control. The subscapularis tendon is felt to be strengthened and stretched by it.
- Step 1: Lay face down on a bench or bed with one arm dangling off the side to begin this exercise.
- Step 2: Raise the relaxed arm straight out and gently until it is parallel to the torso. Hold on for a full minute.
- Step 3: Release to a relaxed posture with gentleness.
- On the other side, repeat. Perform 8 repetitions on each side for 3 sets.
Exercises for Scapular Stabilisation
- This serves to stabilize the scapula.
- This exercise is carried out with the assistance of therapists or other patients.
- The prone position is used for this workout.
- Work out in the I, T, and Y sequence.
- Perform this workout thrice daily, or ten times in one sitting.
Chin-ups.
- As you elevate your chest as high as you can toward the bar, begin with your arms fully extended.
- Hold for a little while at the top, then take a step back to start.
- Finish the five to ten repetitions.
- One set at a time, repeat.
- Everybody works out two or three times a day.
Lateral elevations
- For this workout, start by holding a pair of light dumbbells.
- Your feet are spaced somewhat further apart than the breadth of your hip joints as you stand.
- Make an effort to lift the weights to shoulder level by moving them to the sides.
- It’s important to keep in mind to use your core muscles and gradually reduce the weights to the sides.
- Perform this exercise twice a week for three to four sets of twelve to fifteen reps each.
Abduction combined with internal rotation
- Tie the band firmly above the head and fasten it to the door jamb.
- Avert your gaze from the door.
- Rotate the arm down until the hand is level with the hip while maintaining a 90-degree elbow bend and facing resistance.
Reverse Lawn Mower Starter
- Thera band should be fastened to a doorjamb far above the head.
- As you turn, you should be facing the door.
- Start by extending the arm out to the side and above the head.
- Then, using the opposite motion to start a lawnmower, pull the band up towards the pocket.
Squeeze your shoulder blades
- You are straight on your feet.
- Flex the elbow joint inward and backward.
- bringing the shoulder blades back and downward.
- Then return to your previous position.
- Do this workout three times a day and ten times in a single session.
Raising the shoulders
- You are either seated or standing.
- Start this exercise with your back straight and your arms by your sides.
- Lift your shoulder joint slowly in the direction of your ears.
- After ten seconds of holding this exercise, carefully go back to the beginning position.
- Ten times in a single session and three times a day, repeat this workout.
Shoulder rolls
- Initially Whether sitting or standing, maintain proper posture.
- Next, roll the joint in your shoulders up, back, and down.
- Repeat this exercise ten times.
- After that, roll your shoulder joint ten times in all directions.
- Ten times in a single session and three times a day, repeat this workout.
Wide-legged forward bend in standing
- With your toes pointing forward, you are standing with your feet broader than hip-width. Next, open your chest and interlace your hands behind your back.
- Make use of your leg muscles and maintain a small bend in your knee joint.
- Fold forward by hinging at the hip joint and reaching your arms overhead to the floor.
- Next, lower your chin slightly towards your chest and let your head hang down.
- Ten times in a single session and three times a day, repeat this workout.
T, Y, and I motions
- Stand with your back to a wall and your hands out in front of you.
- Next, carefully raise your arms into a T shape, making sure to maintain touch with the wall with both your arms and your back.
- Following that, keep raising your arms up.
- But it needs to be maintained Put your shoulder blades flat against the wall and concentrate.
- Do all of these exercises three times a day, ten times in each shape.
Cow face Pose
With your hand facing down your spine, begin this exercise by sitting down and raising your left elbow joint to the side of your head.
Draw your left elbow joint to the right by using your right hand to assist you as you slide your hand farther down your spine.
You can also extend your right arm and raise your right hand to grasp your left hand when you’re comfortable doing so.
Maintain the position for a minute.
Do this drill ten times in a single session and three times in a row.
The spinal rolls of Eagle Arms
Stretch your arms out to the sides while seated.
Raise your right arm to the top of your crossed elbows in front of your torso.
After that, bend your elbow joint and bring your hands and forearms together.
To bring your palms together, try extending your right hand around.
For thirty seconds, maintain this posture.
As you draw your elbow joint in towards your chest and exhale, roll your spine.
As you take a breath, expand your chest and raise your arms.
After that, keep up this motion for a minute.
Ten times in a single session and three times a day, repeat this workout.
Swings of the arms over the body
Your feet are hip-width apart when you stand.
Raise your arms to the sides while bringing your shoulder blades together during the inhale.
Gently draw your arms in towards one another as you exhale.
Keep both arms straight while attempting to cross the right arm under the left.
Swing your arms back out to the sides while inhaling and squeeze your shoulder blades together.
Swing your arms gently back towards each other during the exhale.
Keep both arms straight and cross the left arm under the right.
Ten times in a single session and three times a day, repeat this workout.
Safety Points to Remember
The goal of these exercises is to improve the range of motion and lessen shoulder pain.
When performing this workout, make sure to keep the appropriate kind of exercise.
Injuries or pain can result from improper form.
If one is unclear about formation, work with a physical therapist or physician, or observe oneself performing the exercise in a mirror.
If someone is in pain while performing these exercises, reduce the weight and arm movement to a level that is manageable without causing more discomfort.
If the patient’s subscapularis tear discomfort doesn’t go away, they should talk to a physician or physical therapist about other options.
Complication
- Sometimes a tiny tear without surgery might become larger, especially if the muscle has begun to atrophy. Growing old can cause muscle atrophy.
- In addition to causing problems with your biceps, a rupture in the subscapularis muscle can also cause injuries in other rotator cuff muscles. This is due to the fact that other muscles are frequently under a lot of strain and must compensate for a tear in the subscapularis.
Summary
Have you had persistent shoulder pain that just won’t go away? It can be the pain in the subscapularis. The subscapularis muscle, which is located in the shoulder blade, is essential for arm rotation and movement. This muscle can cause chronic shoulder pain if it becomes damaged or inflamed.
The pain in the shoulder blade region is known as subscapularis pain. It may be caused by trauma, overuse, or strain. Pain, weakness, and restricted range of motion are among the symptoms. Medication, physiotherapy, ice application, and rest are all available forms of treatment.
FAQ
When experiencing subscapularis pain, how should one sleep?
When you lie on your back, the injured shoulder won’t be crushed or pushed into an awkward position. Try sleeping in a chair or on a wedge cushion during the first few days or weeks when the symptoms are at their worst. Sleeping on a slight elevation helps keep one from rolling onto their stomach or side while they are asleep.
What is the source of subscapularis pain?
the subscapularis Tendinitis typically results from direct damage to the arm, such as a fall that strikes the arm or shoulders or from an injury sustained during sports. A tendon rupture may also occur following a surgical operation, such as a shoulder replacement, wherein the subscapularis tendon is removed and surgery may done.
What occurs when the subscapularis is tight?
Many issues might arise when the subscapularis becomes weak, tight, or dysfunctional. loss of shoulder range of motion. Sharp and widespread shoulder pain that worsens with activity. Weakness or instability in the shoulder.
What is the subscapularis used for?
The main purpose of the subscapularis muscle is internal rotation, however it can also help with humeral adduction. The muscle is innervated by the subscapularis nerve. Blood is supplied by the subscapular artery, while lymph is drained into the axillary nodes.
How does pain in the subscapularis feel?
Shoulder pain, most especially at the front of the shoulder, is the most common sign of a subscapularis rupture. As someone turns their arm, they may also experience or hear a “clicking” sound in their shoulder. Certain signs of a subscapularis rupture are extremely typical of other symptoms.
References
- Pitcher, V. (2023, October 22). Subscapularis muscle | Best subscapularis exercises. Flawless. https://flawlessphysio.co.uk/subscapularis-muscle/
- Physiotherapy, N. (2023, February 17). Subscapularis- The hidden source of pain – Northwest Physiotherapy Group. Northwest Physiotherapy Group. https://nwpg.com.au/subscapularis-the-hidden-source-of-pain/
- Johnson, K., & Johnson, K. (2023, June 25). Subscapularis Pain: Causes and treatments – One Body LDN. One Body LDN – One Body – One Solution. https://onebodyldn.com/physiotherapy/subscapularis-pain/
- Belly press test. (n.d.). Physiopedia. https://www.physio-pedia.com/Belly_Press_Test
- Thakkar, D. (2023b, March 13). Subscapularis pain – Cause, Symptoms, Treatment, Exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/subscapularis-pain/
- Jyoti. (2022b, July 15). Subscapularis muscle – origin, insertion, function, exercise. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/subscapularis-muscle/
- Subscapularis. (n.d.). Physiopedia. https://www.physio-pedia.com/Subscapularis



One Comment