Scapholunate Dissociation
Scapholunate dissociation is a wrist injury caused by a tear or dysfunction of the scapholunate ligament, leading to instability between the scaphoid and lunate bones. It commonly results from trauma, such as a fall on an outstretched hand, and can cause pain, weakness, and reduced grip strength.
If untreated, it may lead to wrist arthritis. Diagnosis involves clinical examination and imaging, while treatment ranges from splinting and therapy to surgical repair, depending on severity.
Scapholunate Dissociation: What is It?
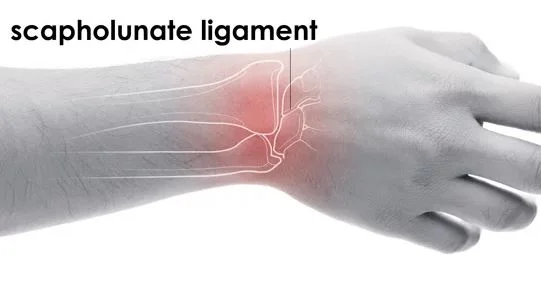
The scapholunate interosseous ligament holds together the scaphoid and lunate bones. This ligament is a robust ring of fibrous tissue that holds them together while permitting controlled movement between them. Scapholunate dissociation is the term for the movement of the bones when this ligament is damaged.
Rotating subluxation of the scaphoid with scapholunate interosseous ligament injury is another name for scapholunate dissociation. X-rays show that the scaphoid and lunate bones are positioned improperly about one another. Your wrist becomes unstable due to the scapholunate ligament tear.
The long-term effects of this damage are significant. The ligament enables the bones to move in unison while holding them together. If the ligament ruptures and does not mend, wrist movements become disorganized, and the joint is impaired. Scapholunate advanced collapse (SLAC), a common form of wrist arthritis, appears if treatment is not received.
The scaphoid and lunate bones might separate from one another due to an unrepaired ligament. The distribution of stresses along the wrists’ numerous joints is changed by this separation. Unusual contact forces cause the cartilage between the different bones to progressively deteriorate. The capitate bone, which is normally found in the lowest row of wrist bones, gradually shifts between the lunate and scaphoid bones. We refer to this motion as the Terry Thomas sign.
Anatomy:
The three physically distinct parts of the C-shaped scapholunate ligament (SLL), often referred to as the scapholunate interosseous ligament (SLIL), are volar, membranous, and dorsal. The strongest and main stabilizing element of the SL joint is the dorsal portion of the SLL, which can withstand stresses of up to 260 N. The volar component of the SLL (118 N) is crucial for rotational stability, but the avascular proximal membranous portion (63 N) offers little discernible laxity control.
Axial stresses are distributed rather uniformly by the carpal bones in the distal row of the carpus; nevertheless, the radio scaphoid joint transmits 50% of an axial force through the wrist, whereas the radio lunate joint transmits 35%. Given that the SLL lies between these two main bones that support weight, it is simple to see how destabilizing damage could happen here.
Several extrinsic ligaments, including the dorsal intercarpal ligaments, scaphocapitate, radioscaphocapitate, and scaphotrapeziotrapezoid, serve as secondary stabilizers.
Midcarpal supination is caused by isometric contraction of the flexor carpi ulnaris, abductor pollicis longus, and extensor carpi radialis longus (ECRL). The volar scaphoid-distal row of the carpus is tightened by midcarpal supination, which stabilizes the scaphoid. Specifically, the flexor carpi radialis (FCR) pronates the capitate and triquetrum and rotates the scaphoid into flexion and supination when loaded. The carpus gains dynamic stability from both of these activities. The stability of the scapula joint is also influenced by proprioception and neuromuscular control.
SLL has a fragile vascular supply, with the radial artery providing the majority of the vascular contribution.
Scapholunate dissociation: what causes it?
The most common cause of SL dissociation is falling on an outstretched hand. Your scapholunate interosseous ligament (SLIL) may be torn by this kind of fall.
Additional reasons for SL separation could be:
- Clutching a steering wheel in a car crash.
- Spastic paraparesis is inherited.
- Congenital ligament laxity, or loose ligaments.
- An inflammatory condition.
Symptoms of Scapholunate Dissociation:
Keep an eye out for the following symptoms, which could indicate scapholunate dissociation, if you have suffered a hand injury or another fall:
- Poor grasp
- The back of your wrist hurts when you grasp
- wrist swelling
- Pain on touching the wrist
- discomfort when you move your wrist backward
- Either clicking or clunking in the wrist
Scapholunate dissociation may occur in whom?
Anyone can be affected by scapholunate dissociation, regardless of gender, color, or ethnicity. However, falling on your hand puts you at the highest risk of developing this condition.
To what extent does scapholunate dissociation occur?
Every wrist sprain involves scapholunate dissociation in approximately 5% of cases. SL separation is seen with around 40% of all distal radius fractures, particularly severe fractures.
The diagnosis of scapholunate dissociation:
You should speak with your physician if you believe your wrist is hurt. To find out what’s happening, they will request X-rays. They might recommend you to an orthopedic surgeon if an x-ray shows a fracture or scapholunate joint enlargement. To identify scapholunate dissociation, a thorough clinical examination and imaging are required. Following an assessment of your wrist’s range of motion, discomfort, and edema your physician might undertake the following:
Test of Scaphoid Shift. When you move your wrist from side to side, your doctor applies pressure on your scaphoid bone to test its stability. When pressure is released, the scaphoid flexes and then snaps back into place if the ligament has ripped.
X-ray. The wider space between the two bones will be visible on an x-ray. The gap is usually a little more than 2 millimeters. Your doctor can assess the alignment of your wrist bones with the use of X-rays taken from various perspectives. If there is a radius fracture, X-rays will also show it.
Magnetic resonance imaging (MRI) scan. Your wrist can be seen in more detail using this imaging technique. The scapholunate ligament tear will be visible to your physician. Additionally, an MRI scan aids in therapy planning.
Arthroscopy. Your doctor inserts a little tube with a light at the end to gain a view of the joint. They could also be capable of doing operations to fix any wounds.
Long-lasting wrist pain might raise your suspicions, particularly if it develops following a fall. Scapholunate dissociation has poor results and may not be completely reversible if left untreated. Because scapholunate dissociation is linked to 10% to 30% of lower radius fractures, your doctor will be notified if they discover one.
Treatment for Scapholunate Dissociation:
Medication will be prescribed by your physician to reduce your discomfort and swelling. To prevent your wrist from moving, they will also put on a splint. Splinting allows the damaged tissues to recover. The bones will revert to their original placements once the ligament heals. Failure to do so could result in long-term harm, which could include:
- Persistent discomfort
- weakened hold
- inflammation of the joints (arthritis)
- Unstable joints
- Advanced collapse of the scapula due to degenerative arthritis
After a few days of treatment, your doctor will request another X-ray to make sure the healing is proceeding as needed. Otherwise, they will suggest surgery to fix the damage.
Surgery for Scapholunate Dissociation:
To do surgery to correct your damage, your doctor might numb your hand and arm. The alternative is general anesthesia, which renders you unconscious. Your wrist will be in a cast for a few weeks following surgery. After that, you will receive physical therapy to strengthen your wrist.
Your ligament might not always be able to be repaired. To join the two bones, your doctor might utilize a portion of the carpi radialis tendon. This tendon connects your hand to the bone of your arm. Arthrodesis, which involves screwing the two bones together, is an additional choice. After closely examining your X-rays and scans, your doctor will determine the best course of action for treating scapholunate dissociation. A stable, pain-free wrist should be the outcome of a successful course of treatment.
Crucial are the scaphoid and lunate bones. Even though there are four wrist bones in the upper row, 35% of the wrist load moves to the lunate, and 50% moves to the scaphoid via the radius. The stability of the hand and wrist can be severely impacted by changes in these bone components’ relative locations. The most common cause of wrist instability is damage to the scapula.
For optimal function restoration, scapholunate ligament injuries must be identified and treated as soon as possible. The most prevalent degenerative arthritis of the wrist, scapholunate advanced collapse (SLAC), is one of the long-term consequences of untreated scapholunate separation.
What steps can I take to lower my chance of scapholunate dissociation?
By taking precautions against falls, you can lower your chance of developing scapholunate dissociation. These actions could consist of:
- Engaging in exercises that enhance your strength, balance, and coordination.
- Preventing trip hazards in your house, such as loose cords, rugs, and dim lighting.
- Utilizing assistive technology, such as a walker or cane, as necessary.
- Putting on stable, flat shoes with adequate traction.
If I have scapholunate dissociation, what can I anticipate?
Complications for SL dissociation could include the following if therapy is delayed:
- Persistent discomfort.
- Inflammatory arthritis.
- Instability of the joints.
- Diminished strength of grasp.
- When degenerative arthritis develops in your wrist, you may have scapholunate advanced collapse wrist.
FAQs
Scapholunate dissociation: what is it?
When the scaphoid and lunate bones in your wrist go out of alignment, it’s known as scapholunate (SL) dissociation. SL separation causes a space to open up between the bones. These bones separate (dissociate) from one another when you move your wrist.
What is the duration of healing for scapholunate dissociation?
It is advised in these situations to immobilize the patient in plaster for four to six weeks, after which analgesics and hand therapy should be administered. It could take up to 18 months to recover.
Is surgery necessary for a scapholunate ligament tear?
Anti-inflammatory drugs or cortisone injections are also frequently used to reduce discomfort. Medication, however, doesn’t deal with the underlying cause of the discomfort and restricted function. You will most likely need surgery to rebuild or repair the ligament if you have suffered a moderate to severe injury.
Is dissociation of scapula a disability?
As previously mentioned, pain, limited mobility, and arthritis are symptoms of the veteran’s scapholunate dissociation handicap, which is currently evaluated as 20% debilitating.
What leads to a tear in the scapula?
The scapholunate joint is a tiny joint that connects the scaphoid and lunate bones, two carpal bones, at the wrist crease. The wrist joint’s stability greatly depends on the scapholunate joint. It is frequently hurt when playing sports, as when you fall hard on your hand.
Are scapholunate wounds self-healing?
Wrist arthritis may result from untreated scapholunate ligaments, which are incapable of healing on their own. The severity of your injury and how long it has been since you suffered it will determine the kind of therapy you receive.
References
- Scapholunate dissociation. (2024, May 1). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/23444-scapholunate-dissociation
- Ankle Sprain vs. Broken Ankle. (2023, April 24). WebMD. https://www.webmd.com/a-to-z-guides/ankle-sprain-vs-broken-ankle