
Pulmonary Rehabilitation
Introduction
Pulmonary rehabilitation is a structured programme designed for individuals with chronic lung diseases like COPD, asthma, or pulmonary fibrosis. It typically includes exercise training, education on lung health, breathing techniques, and psychological support. The goal is to improve lung function, reduce symptoms like breathlessness, enhance quality of life, and promote self-management.
The American Thoracic Society and the European Respiratory Society defined pulmonary rehabilitation in 2013.
In order to improve the physical and mental health of individuals with chronic respiratory diseases and to encourage long-term dedication to health-improving behaviours.
Exercise training, education, and behaviour modification are just a few of the patient-tailored therapies that comprise pulmonary rehabilitation (PR), a comprehensive intervention that begins with a thorough patient assessment.
In order to maximise respiratory function and, consequently, quality of life (QOL) and participation in daily activities, PR is customised for the person who has experienced an exacerbation recently. When compared to standard care, PR has been shown to dramatically increase exercise capacity and health-related quality of life in people with chronic Obstructive pulmonary disease (COPD).
What is PR?
Depending on the resources available, PR programmes differ from person to person and from centre to centre, but generally speaking, they will consist of:
- Multidisciplinary participation
- Exercise
- Nutritional guidance
- Education on disease
- Intervention in psychology
- Intervention through behaviour
In a typical session, a group of individuals with COPD attend a class at a community centre or gym where they engage in supervised exercise under the guidance of a physiotherapist. Following that, they have a lesson with an instructor (usually a nurse or other health care provider) covering a variety of subjects, including managing COPD, stress and anxiety, nutrition, and bronchodilator technique.
A medical programme called pulmonary rehabilitation can help with the symptoms of long-term, chronic lung diseases. A group of medical professionals leads you through exercises (based on your tolerance level), instruction, and breathing management methods for daily tasks.
Your breathing muscles weaken if you have a chronic lung disease. You may be unable to move as much as you would like or used to due to symptoms like shortness of breath. Your symptoms may worsen, and your muscles may become weaker as a result of this vicious cycle. You can resume your activities at your own pace with pulmonary rehabilitation. Although it won’t treat lung disease, you might experience better strength, fewer breathing issues, and an overall higher quality of life.
Anatomy and Physiology
Patients with advanced lung disease have limitations in their ability to work because of problems with gas exchange and alveolar ventilation. Lactic acid accumulation and anaerobic metabolism in the skeletal muscles may result from the consequent reduction in oxygen delivery to the muscles. The fraction of aerobic muscle fibres (Type I fibre) is also reduced, as is the activity of aerobic enzymes.
High-intensity exercise programmes can alter muscle fibre structure and biochemistry at the cellular level, increasing aerobic metabolism and reducing the production of carbon dioxide and lactic acid. This results in improved exercise tolerance and a delayed onset of fatigue.
Types of Pulmonary Rehabilitation Programmes
Outpatient Programme
These are usually carried out in a clinical environment, such as a hospital or rehabilitation facility, where patients go to regular sessions for breathing exercises, education, and supervision.
Inpatient Program
Patients who need more intensive care and are unable to attend outpatient programmes regularly, or who require the best possible medical and ventilatory care, are eligible for inpatient programmes.
Home-Based Programs
These give patients who might have trouble accessing outpatient services flexibility by providing individualised educational and physical activities that are followed at home, frequently under the supervision of medical professionals from home.
Aims
- To lessen the symptoms
- To increase awareness of lung diseases and encourage self-care
- To improve respiratory and peripheral muscle strength and endurance
- To improve exercise tolerance
- To shorten hospital stays
- To assist in improving daily functioning
- To help in the treatment of depression and anxiety
Advantages
- Decrease in the number of hospital days after pulmonary rehabilitation for a year.
- Decrease in the frequency of worsening among patients who exercised daily in comparison to those who did not.
- Decreased episodes following pulmonary rehabilitation
Indications of Pulmonary Rehabilitation
The following chronic lung conditions can benefit from pulmonary rehabilitation:
- COPD (chronic obstructive pulmonary disease)
- Interstitial lung conditions such as pulmonary fibrosis and sarcoidosis
- Asthma
- Cystic fibrosis
- Bronchiectasis
- Pulmonary hypertension
- Lung cancer
- Lung transplant or lung surgery recovery
Risks of pulmonary rehabilitation
The primary risk of pulmonary rehabilitation is that the benefits will start to diminish over time after you’ve finished the programme, which is why it’s crucial to stick to the plan your team develops for you. Your team will closely monitor you to ensure your shortness of breath is manageable, and your muscles may be sore when you first begin the programme, but this should improve with regular exercise.
Complications
The majority of pulmonary rehabilitation complications are caused by poor patient selection. After choosing a patient, a safe and efficient customised plan must be developed. Given that many patients with advanced lung diseases also have heart and musculoskeletal conditions, screening participants for co-morbidities is essential. arrhythmias and cardiovascular ischaemic episodes in at-risk individuals who were not properly screened.
Exercise is necessary to monitor vital signs and oxygen levels, and extra oxygen should be given and gradually decreased as necessary. To prevent falls and injuries, it is important to take into account the patient’s limitations caused by muscle weakness and wasting. Cardiopulmonary exercise testing before enrolment, if it is available, may help reveal underlying musculoskeletal problems, cardiac dysrhythmias, and ischaemia. However, with careful planning, close monitoring, and appropriate patient selection, the majority of complications can be avoided.
Structure
The duration of public relations efforts can range from six to eight weeks to a year. Six to twelve weeks of twice-weekly supervised exercise sessions (plus a third unsupervised session) are advised by the British Thoracic Society’s guidelines , with a minimum of twelve supervised sessions.
PR may be centred in the community, a hospital, or both. The Chronic Respiratory Questionnaire, which assesses emotional function, ability, fatigue, and dyspnoea, indicates that inpatient-based PR produces better results than community-based PR .
Maintenance
Guidelines advise exercise maintenance following PR to sustain improvements in respiratory function, exercise tolerance, and quality of life.
Individuals with moderate-to-severe COPD who participate in a maintenance programme can sustain the improvements they made following an eight-week outpatient PR programme at the two-year follow-up.
Participants in this study showed improved maintenance of their body mass index, 6-minute walk distance, airflow obstruction, dyspnoea score, and exercise capacity scores.
The exercise-focused maintenance programme included home cycle ergometers and, every two weeks, hospital-based supervised exercise sessions. Sixty-six per per cent of the maintenance programme was followed.
Contraindications
- Those who are unable to walk
- Those who have unstable angina
- Individuals who recently suffered a myocardial infarction
Considerations
Other things to think about are :
- Unstable heart disease
- Locomotor problems
- Inability to follow directions because of mental or cognitive impairments
- A support person’s presence to facilitate and promote adherence
Problems secured
- Limitation of ventilation
- More ventilation in dead spaces
- Reduced ability to exchange gases
- Elevated demands on the ventilator as a result of peripheral muscle dysfunction
Limitation of gas exchange
- Reduced strength in the functional inspiratory muscles
- Reduced endurance of the inspiratory muscles
Cardiac dysfunction
- Increased peripheral vascular resistance causes right ventricular afterload.
Skeletal muscle dysfunction
- In moderate to severe COPD, the proportion of type I muscle fibres decreases and the proportion of type II muscle fibres increases at lower work rates compared to age-matched normal subjects.
- The capillary-to-fibre-to-fibre-to-fibre ratio and peak oxygen consumption decrease. Oxidative enzyme capacity decreases and blood lactate levels rise at lower work rates compared to normal subjects.
- Prolonged periods of undernutrition lead to a decrease in strength and endurance.
Respiratory muscle dysfunction
Specific Procedures
In pulmonary rehabilitation, what takes place?
- Exercise
- Education
- Breathing retraining
- Chest physiotherapy and airway clearance
- Mental health support
- Nutrition
Exercise and education are key components of pulmonary rehabilitation. However, your team will customise it according to your objectives and a health evaluation. Among the potential aspects of pulmonary rehabilitation are:
Evaluation
Prior to beginning your programme and following its completion, your healthcare provider will evaluate your:
- Symptoms.
- Oxygen needs.
- Exercise capacity.
- Medical history, including other health conditions (comorbidities).
- Mental health.
They may use questionnaires or tests, such as pulmonary function or stress tests, to evaluate you. They will also discuss your objectives with you. This could include things like visiting family, returning to hobbies, taking short walks, and other activities that would enhance your quality of life.
Exercise
The primary element of pulmonary rehabilitation is physical activity. You will be working out two or three days a week. There will be a provider available to help and guide you. They will choose exercises that are safe for you to do.
It’s likely that you will begin with simple exercises and gradually increase your strength. Depending on your comfort level, each exercise could last a minute or two or as long as thirty minutes. Your healthcare provider will monitor your physical activity level during any exercise and may ask you to rate your level of effort or dyspnoea.
Exercises for pulmonary rehabilitation could include:
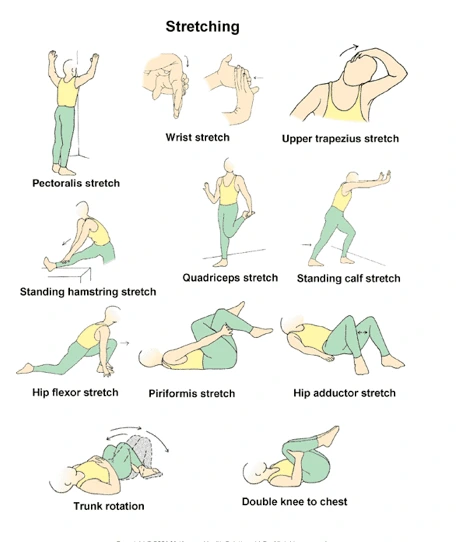
Get warm and cool: Flexibility training
Flexibility training (stretching exercises).
Training of the respiratory muscles: This might involve using a handheld device to forcefully breathe in or out.
Interval or endurance training: This could involve walking, riding a bike, or using a device like a sitting circular.
Weight and resistance training: Light weights, resistance bands, or weight machines can be used for this.
Neuromuscular electrical stimulation through transcutaneous application (NMES): This uses tiny amounts of electricity to contract your muscles.
Education
A healthcare professional will assist you in feeling ready to handle aspects of your life that are impacted by lung disease. This could consist of:
Handling dyspnoea and additional symptoms
Recognising drugs: This covers the side effects of particular medications as well as when and how to use them.
Knowing about oxygen: This covers when to use supplemental oxygen as well as how to check your oxygen level.
Avoiding and managing infections and episodes
Gaining knowledge about using medical equipment at home
Breathing Retraining
A healthcare professional will teach you how to manage and adjust to dyspnoea in your day-to-day activities. This can make regular tasks like cleaning and climbing stairs seem easier. Methods could consist of:
- Controlled breathing methods, such as pursed lip breathing or diaphragmatic breathing
- Methods for relaxation
- Postures that help in the relief of dyspnoea, such as the orthopneic or tripod position.
Airway clearance and chest physical therapy
Your pulmonary rehabilitation program may include airway clearance and chest physical therapy if you have a condition that results in a lot of mucus in your lungs and airways. You can learn from providers how to use tools or methods to remove mucus, such as:
Techniques for breathing and coughing: You can learn methods from a provider to clear your mucus and open your airways. Take huff cough, for example.
PEP stands for positive expiratory pressure: PEP devices hold your airways open and force out mucus by providing resistance, which makes it harder to exhale. Certain PEP devices, such as Flutter, Acapella, AerobikA, and RC-Cornet, oscillate to help break up mucus.
A cappella
Airway clearance vests: An inflatable vest that vibrates to release mucus is called an airway clearance vest or high-frequency chest wall oscillation device.
Percussion and postural drainage: This kind of physical therapy involves shifting into specific positions to allow your lungs to empty. To help release the mucus, someone else places a clap on your back or chest.
Mental health support
Maintaining a chronic health condition can be stressful. You can manage stress, anxiety, depression, and other mental health issues with the following assistance from your care team:
- Distraction and relaxation techniques
- Counselling
- Support communities
- Drugs
Nutrition
Your doctor may recommend certain foods to help you build muscle, depending on the underlying lung condition. This might involve eating smaller but more frequent meals, restricting particular foods, or consuming a specific quantity of protein. In order to lower your risk of aspiration, your healthcare provider might also teach you how to swallow.
How long does a session of pulmonary rehab last?
Sessions for pulmonary rehabilitation typically last one to two hours. Visits with numerous members of your care team who work together with you on various aspects of pulmonary rehabilitation may fall under this category.
Who leads pulmonary rehabilitation?
Your pulmonary rehabilitation team could include:
- Respiratory therapists
- Physical therapists
- Occupational therapists
- Pulmonologists
- Psychologists
- Dietitians
- Social workers
What is the duration of pulmonary rehabilitation?
For four to twelve weeks or longer, pulmonary rehabilitation typically takes place two or three times per week. To keep getting the benefits of pulmonary rehabilitation, you must engage in safe physical activities at home.
Can pulmonary rehabilitation improve your lungs?
Yes, pulmonary rehabilitation can help you improve the function of your lungs. Although it won’t treat lung disease, it can lessen its symptoms, such as coughing and dyspnoea.
To what extent does pulmonary rehabilitation work?
When compared to those who have not, individuals with chronic lung disease who have finished a pulmonary rehabilitation programme have:
- Reduced chance of readmission to the hospital.
- An enhanced ability to exercise.
- Improved quality of life in relation to health.
- Breathlessness has decreased.
- Following the programme, you should continue to perform the exercises and apply the skills you have learnt to get the most out of pulmonary rehabilitation. A long-term plan will be created for you by your team.
How can pulmonary rehabilitation benefit me the most?
Here are some pointers for making the most of pulmonary rehabilitation and ensuring its success:
- Share your programme completion objectives with your providers. As you progress through the programme, keep these objectives in mind.
- Tell your providers the truth. If any activity is excessive, let them know. Share your feelings with them regarding your progress so far.
- Think about what will facilitate—or even enjoy—exercise and other forms of therapy for you. This could involve using a fan, music, outdoor workout equipment, apps that track your activity or provide exercise instructions, and more.
- Enquire about any other medical equipment that might be useful, such as a walker.
- Participate in each session: If you don’t finish the entire programme, you won’t get as much benefit.
- Inform your loved ones about how they can help you make the most of the programme.
Intervention
Physiotherapists are crucial in the prescription, monitoring, and evaluation of exercise results. It indicates that the use of the FITT methodology—which stands for frequency, intensity, time, and type—to prescribe exercises based on guidelines has increased. When compared to usual care, participants who engage in both functional and maximal exercise exhibit statistically significant improvements following PR.
Pulmonary care: positioning, exercises, bronchodilator, etc.
Functional training: Important in cases of severe fatigue, weakness, or end-stage illness
- Adapt the environment to improve ease.
- Work areas supported in places that are easy to avoid bending
- Find a table where you can slide bulky items while working.
- In addition to bathtubs, there are chairs at stair landings.
- Making use of assistive technology and adaptive equipment
- Using adequate ventilation in areas with fumes, such as kitchens
Altering performance tasks:
- Slow pace
- Minimise large body movements.
- Plan tasks including breaks and rest
Include techniques to reduce symptoms.
- Continue breathing normally without using Valsalva.
- Don’t talk too much while working on a task.
- Elderly people with obstructive lung disease may lean forward and pace when lifting objects, which raises intra-abdominal pressure, encourages the diaphragm to rise in a more favourable position, and enables the accessory muscles of inspiration to draw the chest into inspiration.
- Rapid shallow breathing is easier in restrictive lung disease because the respiratory system’s elastic resistance is avoided.
- Using biofeedback to relax non-respiratory muscles lowers anxiety associated with dyspnoea.
Particular Exercise Program
Progressive resistance training and supervised aerobic exercise should be part of any exercise programme. Individual exercise recommendations should be made based on the results of the initial evaluation, and objectives should be decided upon.
Regular monitoring of participants’ exertion is necessary, with special attention paid to any chest pain, discomfort, or dyspnoea.
For mild lung disease
- Have symptoms with extreme effort (cough, sputum)
- According to spirometry, the expected vital capacity (VC) is 70–80%, and the forced expiratory volume in the first second (FEV1) is 70–80%.
- ABG: normal, mild hypoxaemia
- Individual exercises are suggested, exercise testing and training take place, and official rehabilitation is not necessary.
For moderate lung disease
- Shortness of breath during everyday activities is common in subjects with moderate lung disease.
- When pulmonary disease is detected following major surgery, an episode of acute pneumonia occurs, and PR shows promising outcomes.
- VC and FEV1 55-70% (indicates shortness of breath at approx. 3-4 METS)
- Exercise testing: start at a low metabolic equivalent (MET), i.e., 1.5 MET, and progress 0.5 MET at each stage, monitoring ECG, BP, and HR, or perform a 12-minute walk test.
Exercise prescription:
- Intensity: HR at a point on the Borg’s scale of perceived exertion when the patient is 2-3 dyspnoeic
- Frequency: 5-7 times a week
- If symptoms develop, use oxygen.
For Severe Lung Disease
- Breathlessness during most everyday activities
- VC and FEV1 <50%
- Needs oxygen at rest
- Some show R ventricular dysfunction
- Testing: low-level intermittent tests or exercises set at a steady endurance test of 2-3 METs
- Training: interval training, short exercise bouts, frequent rests, once a day, when duration increases to 20 mins, 5 times a week
- Intensive monitoring
- When monitoring oxygen, every decrease in SPO2 of 3% should be noted. If the drop reached <88% SPO2 oxygen therapy is indicated.
Steps to Setting Up an Exercise Class
1) Understand your limits
Make sure you possess the information and abilities necessary to instruct, encourage, and inspire the students in your classes.
2) Determine unique selling point and product
Exercises of various kinds are helpful for patients with pulmonary diseases, and patients are frequently drawn to particular exercises. Aerobic exercises like walking, cycling, or rowing could be included in this.
On the other hand, some people prefer multi-exercise pursuits like cross-training or high-interval intensity training, being outside, or honing skills like dancing or hiking.
Find a specific that will attract clients in your target location, and encourage them to stay
3) Build intensity level
Start at a low duration, reps, sets and load.
Encourage patients to listen to their body and slowly build
Clinical Importance
A variety of measurements are used to assess the pulmonary rehabilitation programme’s benefits. The majority of the initial investigations into pulmonary rehabilitation involved patients with COPD. However, patients with various lung diseases are also undergoing pulmonary rehabilitation, and the underlying disease process may naturally influence the results.
One of the key outcomes examined in pulmonary rehabilitation is the benefit to survival. Others have contested the finding that pulmonary rehabilitation that begins within three months of hospital discharge has a lower one-year mortality risk.
Exercise capacity and quality of life are significant measurements that can be assessed. It has been demonstrated that pulmonary rehabilitation enhances quality of life as assessed by the Chronic Respiratory Disease Questionnaire (CRQ) and St George’s Respiratory Questionnaire (SGRQ).
Given that smoking accounts for the majority of COPD cases and plays a part in the disease’s progression, pulmonary rehabilitation programmes offer a special chance to address quitting smoking. Positive reinforcement has the effect of motivating smokers to quit in a rehabilitation setting.
A common component of the programme’s action plan is quitting smoking. Patients can also participate in advanced care planning because pulmonary rehabilitation offers a variety of disciplines. It was possible to have an improved advanced care conversation with patients who were participating in pulmonary rehabilitation.
FAQs
How does pulmonary rehabilitation work?
A structured exercise program called pulmonary rehabilitation (PR) is intended for individuals with long-term lung conditions such as pulmonary fibrosis (PF). Exercise training, breathing techniques, managing stress, anxiety, and depression, dietary counseling, education, and more are all part of pulmonary rehabilitation.
What are the pulmonary rehabilitation principles?
The use of assisted ventilation, medication and oxygen delivery, patient education, nutritional management, and rehabilitation therapies are all essential elements of a pulmonary rehabilitation program. This chapter reviews common conditions that cause pulmonary dysfunction as well as rehabilitation techniques.
For whom is pulmonary rehabilitation appropriate?
All of the following requirements must be fulfilled by the patient: Chronic respiratory conditions that cause dyspnea that impairs functional ability, such as pulmonary fibrosis, bronchiectasis, and COPD (usually MRC 3 or more) best possible medical care. capable of walking five meters on their own (with or without walking aids)
What are pulmonary rehabilitation’s three main objectives?
Pulmonary rehabilitation’s three primary objectives are to assist you in:
Discover how to control your illness.
assist you in feeling better.
Make long-term lifestyle adjustments.
What tools are employed in the field of pulmonary rehabilitation?
The majority of pulmonary rehabilitation programs are held in hospital gymnasiums and may involve resistance training with weight machines, aerobic training with treadmills, stationary cycles, and arm and rowing ergometers.
For whom is pulmonary rehabilitation inappropriate?
People with unstable heart disease, neurological conditions that prevent them from exercising, such as severe peripheral vascular disease or arthritis, those nearing the end of their illness, or those with severe cognitive or mental impairment should not undergo pulmonary rehabilitation.
Reference
- Professional, C. C. M. (2025c, March 19). Pulmonary rehabilitation. Cleveland Clinic. https://my.clevelandclinic.org/health/treatments/pulmonary-rehabilitation
- Wikipedia contributors. (2024, September 14). Pulmonary rehabilitation. Wikipedia. https://en.wikipedia.org/wiki/Pulmonary_rehabilitation



One Comment