Proximal Radioulnar Joint
The proximal radioulnar articulation, sometimes referred to as the proximal radioulnar joint (PRUJ), is a synovial pivot joint that occurs between the ring created by the annular ligament and the radial notch of the ulna and the circumference of the radius head.
Introduction
A synovial joint that joins the proximal ends of the radius and ulna is called the proximal radioulnar joint. The annular ligament and the radial notch of the ulna form a ring that contains the circumferent head of the radius in this joint. This joint is a pivot joint due to its configuration.
Being a uniaxial joint, the proximal radioulnar joint can move with only one degree of freedom, from pronation to supination. This movement is specific to the human upper limb.
Structure
The proximal radioulnar joint is a pivot joint made of synovium. It happens between the radius’s head’s circumference and the ring that the annular ligament and the ulna’s radial notch make. The forearm’s interosseous membrane and the annular ligament stabilize the joint.
The PRUJ is created by the ulna’s radial notch articulating with the medial side of the radial head. The PRUJ is stabilized by several ligaments during movement.
Near the proximal radioulnar joint are several nerves, including:
- Median nerve
- Musculocutaneous nerve
- Radial nerve
Embryology
Shh secretion by the notochord controls the formation of the upper limb bud, which begins 26 days after fertilization.
The bud’s lateral plate mesoderm creates the joint’s bone, cartilage, and tendon. These cells develop into chondrocytes and osteoblasts after the mesenchyme condenses into a blastema in the limb bud core. Proximally, the upper limb begins to chondrify at 36 days.
At the locations of future joints, chondrification is suppressed. Studies have shown that these interzones express the proteins GDF5, WNT1, and WNT14. The annular ligament and proximal radioulnar joint interzone develop 51 days following fertilization. The formation of the articular cavity starts 56 days after fertilization. In the eleventh week, the elbow starts to mature. By week 12, the quadrate and annular ligaments are well-defined.
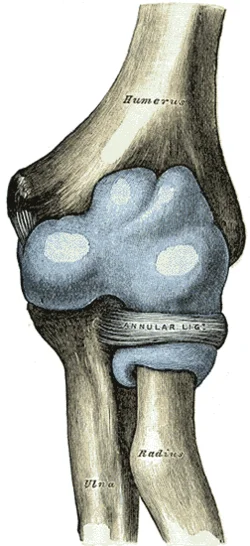
Articular surfaces
The radial fossa of the ulna and the head of the radius are the articular surfaces of the proximal radioulnar joint.
Hyaline cartilage lines on both surfaces. While the radial fossa is reciprocally concave, the radial head is round and convex.
The radial fossa, however, only touches one-fifth of the radial head. To ensure the completeness of this pivot joint, the radial head is tightly held against the ulna’s radial fossa by the annular ligament.
Joint capsule
The joint capsule, which surrounds the elbow joint, is continuous with the synovial membrane. The anterior portion of the capsule, which attaches the medial epicondyle and ulnar coranoid process anteriorly, makes it comparatively slender in comparison to other capsules. The capsule’s posterior part is thinner than its prior part.
Ligaments
Proximally, the fibrous capsule of the radioulnar joint is continuous with the capsule of the elbow joint, but distally, it links to the annular ligament. The articular surface margins and the annular ligament are where the synovial membrane is attached. Along the inside of the capsule, it forms a continuous line with the elbow joint’s synovial membrane. Therefore, there is a single, continuous synovial cavity shared by the elbow and proximal radioulnar joints.
The quadrate and annular ligaments support the proximal radioulnar joint.
- Annular ligament: robust ligament that is connected to the front and back of the ulna’s radial notch. The head of the radius is surrounded by it and the ulna’s radial notch.
- Ulnar collateral ligament
- Radial collateral ligament
Annular ligament
After encircling the radial head and attaching to the posterior margin of the radial fossa, the annular ligament extends from the anterior margin of the ulna’s radial fossa. The radial head can spin within this stable ring, which is made possible by the annular ligament.
While the ligament’s distal boundary affixes to the radius’s neck, its proximal margin is fused with the joint capsule. The surface of the radius is directly in contact with the thin layer of cartilage covering the internal surface of the annular ligament. The supinator muscle attaches to the superficial surface, which is united with the radial collateral ligament.
A brief fibrous band called the quadrate ligament extends from the neck of the radius, directly in front of the radial tuberosity, to the superior portion of the supinator fossa of the ulna.
Interosseous Membrane
A band of connective tissue called the interosseous membrane connects the ulna and radius between the radioulnar joints.
The lateral ulnar border and the medial radial border are separated by it. The sheet has tiny pores that serve as a channel for the blood vessels in the forearm.
Three main purposes are served by this connective tissue sheet:
- Adds stability by holding the ulna and radius together when the forearm is pronated or supinated.
- Serves as a point of attachment for the forearm’s anterior and posterior muscles.
- Transmits forces to the ulna from the radius.
Innervation
The branches of the ulnar, radial, musculocutaneous, and median nerves supply the proximal radioulnar joint.
Blood supply
The deep brachial artery’s radial collateral branch, as well as the radial and recurrent branches of the radial and common interosseous arteries, create the periarticular network that supplies blood to the proximal radioulnar joint.
Blood is supplied to the upper extremities by the brachial artery, which splits at the proximal cubital fossa into the radial and ulnar arteries. Medial, lateral, and posterior arcades are formed around the elbow by branches of the brachial, radial, and ulnar arteries. The proximal radioulnar joint is supplied by the lateral arcade of these arcades.
The radial recurrent artery and the interosseous recurrent artery anastomose with the radial and middle collateral arteries from the profunda brachii artery form the lateral arcade. The radial head and neck are perfused by the radial and interosseous recurrent arteries, while the intraosseous branch of the ulnar artery supplies blood to the proximal ulna.
Lymph is drained from deep lymphatic vessels in the palm by the radial and ulnar lymphatic vessels (RLV, ULV), which are deep lymphatic vessels of the forearm. This anterior interosseous lymphatic vessel, which originates in the pronator quadratus, drains into the cubital fossa as the ULV continues proximally towards it. The lymph of the RLV and ULV enters the cubital fossa, drains into the cubital lymph nodes, and then enters the brachial lymphatic vessel (BLV). Proximally, the BLV continues and enters the axillary lymph nodes.
Nerves
The PRUJ shares innervations with the humeroulnar and humeroradial joints because they share a joint capsule. The elbow capsule’s innervation is separated into anterior and posterior capsules.
A tiny branch of the musculocutaneous nerve makes its way to the anterior capsule’s center via the brachialis muscle. The branch overlaps with the medial and radial nerves in certain places as it moves laterally and medially, respectively.
The median nerve innervates the medial part of the anterior capsule through tiny branches it produces before passing the pronator teres. Additionally, a branch from the median nerve may emerge just proximal to the elbow and descend to the anterior capsule. The radial nerve branch that innervates the posterior capsule also innervates the lateral part of the anterior capsule.
The radial nerve travels down the lateral head of the triceps and innervates the lateral part of the posterior capsule. After passing through the supinator muscle, it innervates the anterior capsule as well. The medial part of the posterior capsule, which surrounds the medial epicondyle and olecranon, is innervated by joint branches of the ulnar nerve that emerge just above the cubital tunnel. The central part of the posterior capsule receives innervation from the radial and ulnar nerves that overlap.
Muscles
Pronation and supination are the PRUJ’s main movements, and they happen in tandem with the distal radioulnar joint.
The pronator teres and pronator quadratus are the forearm’s two main pronators. The humeral head of the pronator teres originates on the medial epicondyle, while the ulnar head is derived from the coronoid process. These heads unite before inserting onto the mid-radius lateral surface. The pronator quadratus is connected to the lateral radius and the distal quarter of the anterior ulna. The median nerve innervates both the quadratus and the pronator teres from levels C6-7 and C8-T1, respectively.
The main forearm supinators are the supinator and biceps brachii muscles. The long and short heads of the biceps brachii originate from the coracoid process and supraglenoid tubercle, respectively, and cover two joints. The heads then attach to the medial part of the radial tuberosity and the anterior capsule via the distal biceps tendon and the bicipital aponeurosis, respectively.
The biceps can flex the elbow and supinate the forearm thanks to these attachments. From nerve root levels C5–6, the musculocutaneous nerve innervates the biceps muscle. The anterior proximal ulna, lateral epicondyle, RCL, and annular ligament are the origins of the supinator. The dorsolateral proximal radius is where it inserts after encircling the radius. The radial nerve innervates it at nerve root level C6.
Movements
To allow for forearm rotation, including pronation and supination, the proximal and distal radioulnar joints function as a single unit. Pronation and supination ranges of motion are 61–66° and 70–77°, respectively, while the arm is lying next to the torso.
The head of the radius rotates inside the ring that the radial fossa and annular ligament form in the proximal radioulnar joint. The location of the forearm determines the dynamic axis of rotation. The axis goes through the ulnar attachment of the articular disc in the distal radioulnar joint and the center of the head of the radius proximally when the forearm is in a supinated position. The distal end of the axis travels medially and passes through the ulna’s head when the forearm is pronated.
Supination and pronation are followed by a series of additional motions in the proximal radioulnar joint in addition to the rotation of the radial head;
- The superior surface of the radial head revolves in opposition to the humeral capitulum.
- The ridge of the radial head slides against the humeral capitulum-trochlea groove.
- Laterally and inferiorly, the head of radius tilts in the transverse plane.
- The radial head is displaced laterally because the ellipsoid cross-section of the radius causes its broader axis to enter a transverse plane.
When the supination angle is 5°, the proximal radioulnar joint assumes a closed-packed configuration. The forearm is in the open-packed (resting) posture when it is flexed at 70° and supinated at 35°. Pronation and supination define and restrict the joint’s capsular arrangement. The supplementary movements of the anteroposterior gliding of the radial head against the ulna and the humeral capitulum are made possible by the proximal radioulnar joint.
Muscles acting on the proximal radioulnar joint
The pronator quadratus and pronator teres are the muscles that work on the proximal radioulnar joint to cause pronation. The pronator teres is involved in rapid movements and movements against resistance, whereas the pronator quadratus is sufficient for little motions.
The contraction of the supinator muscle during forearm extension results in supination. During resistance exercises and/or forearm flexion, the biceps brachii muscle serves as an accessory supinator.
Clinical significances
A Monteggia fracture occurs when the radial head dislocates and the ulna fractures at the same time. Although these fracture patterns can happen to adults, they are most frequently seen in children aged 4 to 10. Although olecranon fracture-dislocation and radial head fracture-dislocation variant patterns are also recognized, the ulnar fracture conventionally occurs distal to the olecranon, and the dislocation involves both the PRUJ and the radiocapitellar joint.
There are four types of Monteggia fractures. Forced pronation of the forearm, such as falling on an extended and pronated upper limb, is the most common cause of the injury. The most prevalent is type I, in which the ulna’s diaphyseal fracture occurs along with an anterior dislocation of the radial head. Type II posterior dislocation of the radial head frequently exhibits a concomitant radial head fracture.
Children who have an ulna metaphyseal fracture and either a lateral or anterolateral radial dislocation are most likely to experience type II. Finally, an anterior dislocation that includes a proximal third of the radius fracture and an ulna diaphyseal fracture is a type IV. Restoring motion can be accomplished through principal treatment using open reduction and internal fixation (ORIF).
Children can also develop a nursemaid’s elbow, a dislocation of the radial head without a concomitant fracture. When the forearm is pulled axially, the radial head subluxes outside the annular ligament, which becomes positioned between the radial head and capitellum. This is a common consequence of this subluxation. Isolated radial head subluxation is significantly less frequent in children older than five as the annular ligament’s structural integrity increases and becomes thicker.
Pediatric patients typically arrive with their arms held in a slightly flexed and slightly pronated position. Both the hyperpronation technique and the supination and hyperflexion maneuver, which apply the thumb reduction force over the radial head, are examples of reduction techniques. Although rare, recurrence is possible, particularly in patients under three. For initial events, immobilization is not required. Consider cast immobilization with the arm held in flexion and in a neutral to slight forearm supination position if recurrence is observed several times in a short time.
FAQs
The proximal radioulnar joint: what is it?
The proximal ends of the radius and ulna are joined by a synovial joint called the proximal radioulnar joint. The annular ligament and the radial notch of the ulna form a ring that contains the circumferent head of the radius in this joint. This joint is a pivot joint due to its configuration.
Which joint type is the proximal joint?
The articulation between the hand’s proximal and middle phalanx is known as the proximal interphalangeal joint (PIPJ). All fingers except the thumb have it. Fine motor control is aided by this synovial hinge joint, which allows for flexion and extension in the middle of the fingers.
Which ligament is the most crucial component of the proximal radioulnar joint?
A sequential transection of the soft tissue constraints of the proximal radioulnar joint revealed that the central band of the interosseous membrane and the annular ligament serve as the primary stabilizers in pronation, while the central band is the major stabilizer in supination.
What is the proximal radioulnar joint used for?
The ulna on the medial side and the radius on the lateral side are the two forearm bones that connect to form the radioulnar joints. Pronation and supination are made possible by the combined action of the superior, or proximal, and inferior, or distal, radioulnar joints.
Which two bones make up the joint between the proximal radioulnar bones?
Immediately distal to the elbow joint, and contained within the same articular capsule, is the proximal radioulnar joint. The radial notch of the ulna and the head of the radius articulate to form it.
Which rule of the proximal radioulnar joint is concave-convex?
According to the convex-concave rule, rolling and gliding happen in opposite directions during forearm pronation and supination when the convex radial head articulates with the concave radial notch on the ulna. This is thought to be the case with the arthrokinematics of the proximal radioulnar joint (PRUJ).
What is the proximal ligament of the radioulna?
The proximal radioulnar joint is a pivot joint made of synovium. It happens between the radius’s head’s circumference and the ring that the annular ligament and the ulna’s radial notch form. The joint is stabilized by the annular ligament and the forearm’s interosseous membrane.
At the proximal radioulnar joint, which muscles are present?
Pronator teres muscle.
Flexor carpi radialis muscle.
Palmaris longus muscle. palmar aponeurosis.
Flexor carpi ulnaris muscle.
What distinguishes the distal radioulnar joint from the proximal one?
Together with the humeroulnar and humeroradial joints, the proximal radio-ulnar joint (PRUJ) makes up the elbow’s articulating components. Pronation and supination of the forearm are made easier by the PRUJ, which is situated in the proximal forearm and works in tandem with the distal radio-ulnar joint (DRUJ).
How does the proximal radioulnar joint look clinically?
The proximal ends of the radius and ulna are joined by a synovial joint called the proximal radioulnar joint. In this joint, the annular ligament and the radial notch of the ulna form a ring that contains the circumferent head of the radius. This joint is a pivot joint because of its configuration.
What are the proximal radioulnar joint landmarks?
The radioulnar joint at the proximal end is a synovial pivot joint. It is situated between the ring created by the annular ligament the radial notch of the ulna and the circumference of the radius head. The joint is stabilized by the annular ligament and the forearm’s interosseous membrane.
What is the proximal radioulnar joint also known as?
The synovial pivot joint between the radius’s head circumference and the ring created by the ulna’s radial notch and the annular ligament is called the proximal radioulnar articulation, or proximal radioulnar joint (PRUJ).
References
- TeachMeAnatomy. (2020b, November 7). The Radioulnar Joints – TeachMeAnatomy. https://teachmeanatomy.info/upper-limb/joints/radioulnar-joints/
- Proximal radioulnar joint. (2023, November 3). Kenhub. https://www.kenhub.com/en/library/anatomy/proximal-radioulnar-joint
- Wikipedia contributors. (2025, January 11). Proximal radioulnar articulation. Wikipedia. https://en.wikipedia.org/wiki/Proximal_radioulnar_articulation
- Williams, M. R., & Varacallo, M. A. (2023, July 24). Anatomy, shoulder and upper limb, proximal Radio-Ulnar joint. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK551614/
- Hacking, C., & Stewart, M. (2017). Proximal radioulnar joint. Radiopaedia.org. https://doi.org/10.53347/rid-53632