Intercostal Nerves
Introduction
The intercostal nerves are a group of 11 pairs of nerves that originate from the thoracic spinal cord (T1 to T11). They run between the ribs, supplying the muscles of the chest wall and providing sensory information from the skin and pleura. The 12th pair, called the subcostal nerve, runs below the last rib. These nerves play a key role in breathing by controlling the intercostal muscles.
Both motor and sensory fibers are carried by the intercostal nerves, which are mixed nerves. Their primary role is to supply the abdominal and thoracic wall structures with segmental supply. They transport sensory afferents from the skin of the thoracic and abdominal wall, ribs, pleura, and peritoneum in addition to their motor innervation for the intercostal muscles and the muscles of the anterolateral abdominal wall. Additionally, these nerves provide sympathetic innervation to the thoracic and abdominal wall structures (blood vessels, sweat glands).
There are twelve pairs of thoracic spinal nerves located in the thoracic portion of the spinal cord. 11 intercostal nerves are derived from the anterior/ventral rami of the first 11 thoracic spinal nerves. The subcostal nerve is the name given to the twelfth nerve since it is situated inferior to the final rib.
Pre- and postganglionic branches (rami communicantes) link each intercostal nerve to its associated sympathetic ganglion (of the sympathetic trunk) during arising. Then, between the parietal pleura and the posterior (internal) intercostal membrane, the intercostal nerves enter the appropriate intercostal gap.
Structure
The associated intercostal gap between the parietal pleura and the posterior intercostal membrane is where each intercostal nerve enters. At this location, the intercostal nerve is just outside the parietal pleura before plunging into the rib’s subcostal groove, which is located directly beneath the rib.
The innermost intercostal muscle and the interior intercostal muscle enclose the nerve as it passes through the subcostal groove. The matching intercostal gap, directly beneath the corresponding rib, is where the first six intercostal nerves terminate after branching off. After leaving the intercostal gaps, the seventh through eleventh intercostal nerves enter the abdominal wall. Because of this trajectory, the final five intercostal nerves are known as thoracoabdominal nerves.
Intercostal nerve 1
Around the neck of the first rib, the anterior ramus of the first thoracic spinal nerve splits into superior and inferior branches, marking its termination.
The bigger, superior branch joins the brachial plexus after leaving the thoracic cavity. The first intercostal nerve is the inferior branch, sometimes referred to as the intercostal branch.
This nerve terminates as the first anterior cutaneous branch on the anterior chest wall after passing through the first intercostal gap, which lies beneath the first rib.
Intercostal nerves 2-6
Between the posterior intercostal membrane and the parietal pleura, the anterior rami of the second, third, fourth, fifth, and sixth thoracic spinal neurons enter their respective intercostal spaces directly. Between the internal intercostal muscles and the innermost intercostal, these nerves continue anteriorly.
These nerves run inferior to the intercostal artery and vein, passing inside or slightly below the costal groove as they travel through the intercostal region. Each of these nerves produces lateral cutaneous branches close to the midaxillary line. The intercostal nerves terminate by piercing the internal intercostal muscles and external intercostal membranes between the costal cartilages and the pectoralis major muscle to become anterior cutaneous branches at the anterior chest wall, near the sternum. They also pass anterior to the internal thoracic vessels.
The floor of the axilla and the upper posteromedial portion of the upper extremity are supplied by the intercostobrachial nerve, which is the lateral cutaneous branch of the second intercostal nerve. Patients with acute coronary artery disorders, such as heart attacks, typically have left-sided arm and axillary discomfort. The intercostobrachial nerve mediates this cardiac-referred discomfort.
Intercostal nerves 7-11
Additionally, the anterior rami of the final five spinal neurons (the seventh, eighth, ninth, tenth, and eleventh) enter and travel through the appropriate intercostal gaps. Here, they feed the intercostal muscles and the thoracic wall.
But after passing through the intercostal gaps, the nerves pierce the anterior rectus sheath and proceed behind the costal border into the abdomen wall, where they end as anterior cutaneous branches. The parietal peritoneum and the skin and muscles in this area are supplied by these intercostal nerves. The thoracoabdominal nerves are another name for these nerves since they innervate both the thoracic and abdominal walls.
Dermatomes
The region of the skin where sensory nerves originate from a single spinal nerve root is known as a dermatome. T1–T12 are the dermatomes associated with the abdomen and thorax.
Each is quite uniformly spaced anteriorly, and the lines T1–T6 are almost horizontal and cross the thoracic wall.
Additionally, the thoracic wall is where the dermatomes T7–T12 begin horizontally, but they have a tendency to dip inferiorly and extend onto the abdominal wall beforehand.
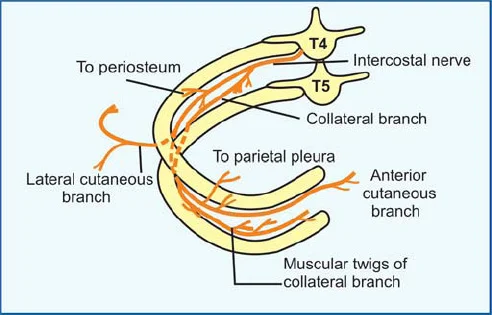
Branches
Intercostal nerves are usually mixed nerves that innervate the thoracic and abdominal walls both motorly and sensoryly. Typically, the nerves produce several branches as they travel:
The muscular branches for the levatores costarum, transversus thoracis, serratus posterior superior, intercostal, and subcostal muscles.
In addition to the anterior cutaneous branches, which further split into medial and lateral branches, the lateral cutaneous branches also split into anterior and posterior branches. The skin of the anterolateral walls of the abdomen and thorax receives segmental sensory innervation from these branches.
The collateral branches innervate the periosteum of the rib, the parietal pleura, and the intercostal muscles. They originate near the angles of the ribs and go along the superior border of the inferior rib.
The ipsilateral sympathetic trunk and each intercostal nerve are connected by the communicative branches, or rami communicantes. Postsynaptic fibers return from the ganglions to the closest anterior rami of spinal nerves, whereas presynaptic fibers travel from the anterior rami of the spinal nerves to the trunks. The blood vessels, sweat glands, and smooth muscle of the body wall and limb are then innervated by the sympathetic fibers after they have passed via the intercostal nerves.
Clinical Importance
Intercostal neuralgia is the term used to describe pain that originates from the intercostal nerves. A frequent condition known as intercostal neuralgia can be caused by herpes zoster, trauma, nerve entrapment, and chronic nerve irritation. Intercostal neuralgia patients report their pain as intense, searing, or shooting. Usually, the discomfort starts at the posterior axillary line and moves anteriorly into the intercostal nerve’s distribution zone.
Those who do not take enough breaths have complications since the discomfort might be replicated after deep inhalation or other chest wall motions. Treatment options for intercostal neuralgia include non-somatic therapy, interventional pain management, and pharmaceutical therapy with tricyclic antidepressants or anticonvulsants.
Intercostal nerve blocks are a good way to provide analgesia, but because of their proximity to the pleural space, technique, and anatomy must be carefully considered. The architecture of the intercostal nerves and the vasculature that surrounds them must thus be well understood by medical professionals doing such treatments.
Surgical Importance
During thoracotomy surgeries, the intercostal nerves are always at risk of injury. During the insertion of a chest tube, the intercostal nerves are potentially susceptible to injury or transection.
In contrast to a stab insertion, there have been case reports detailing chest tube installation methods that involve meticulous dissection of the intercostal areas and identification of the intercostal nerve. Additionally, anesthetic blocks of the intercostal nerves before thoracotomy closure have been reported to cause hypotension in both cases with and without a spinal block.
FAQs
How to stop intercostal nerve pain?
Some options to treat intercostal neuralgia are:
Non-steroidal anti-inflammatory drugs (NSAIDs)
Antidepressant or anticonvulsant medication.
Intercostal nerve block.
Radiofrequency lesioning.
Occupational therapy.
Physical therapy.
Cognitive or behavioral therapy.
Surgery.
What irritates intercostal nerves?
Your intercostal nerves, which are located just beneath your ribs, can become irritated, inflamed, or compressed, resulting in intercostal neuralgia. This can be caused by several factors, including chest trauma. viral infections, such as shingles.
How do you sleep with intercostal nerve pain?
Back sleepers should cushion their upper back by holding a body pillow to their chest, while side sleepers should avoid resting on the side that is strained and put a pillow between their knees. Many individuals struggle to get to sleep and remain asleep.
Can anxiety cause intercostal pain?
Hyperventilation during panic attacks may lead to musculoskeletal chest pain, with strain or spasms of intercostal chest wall muscles. Esophageal dysmotility can be caused by acute anxiety this dysmotility may lead to esophageal spasm, a well-described cause of noncardiac chest pain.
Can intercostal nerve pain go away?
Intercostal Neuralgia: Does It Go Away? Depending on the underlying cause, intercostal neuralgia may go away with treatment in a few weeks to months. Furthermore, symptoms could disappear on their own without medical help. Conversely, some people will experience chronic pain for a very long period.
References
- Intercostal nerves. (2023, October 30). Kenhub. https://www.kenhub.com/en/library/anatomy/intercostal-nerves
- Intercostal nerves. (2023, May 22).StatPearls.https://www.ncbi.nlm.nih.gov/books/NBK538238/