Wrist Joint
Introduction
The wrist joint, also known as the radiocarpal joint, is a complex structure that connects the hand to the forearm. It is responsible for a wide range of movements, including flexion, extension, radial deviation (movement toward the thumb), ulnar deviation (movement toward the little finger), and some degree of circumduction.
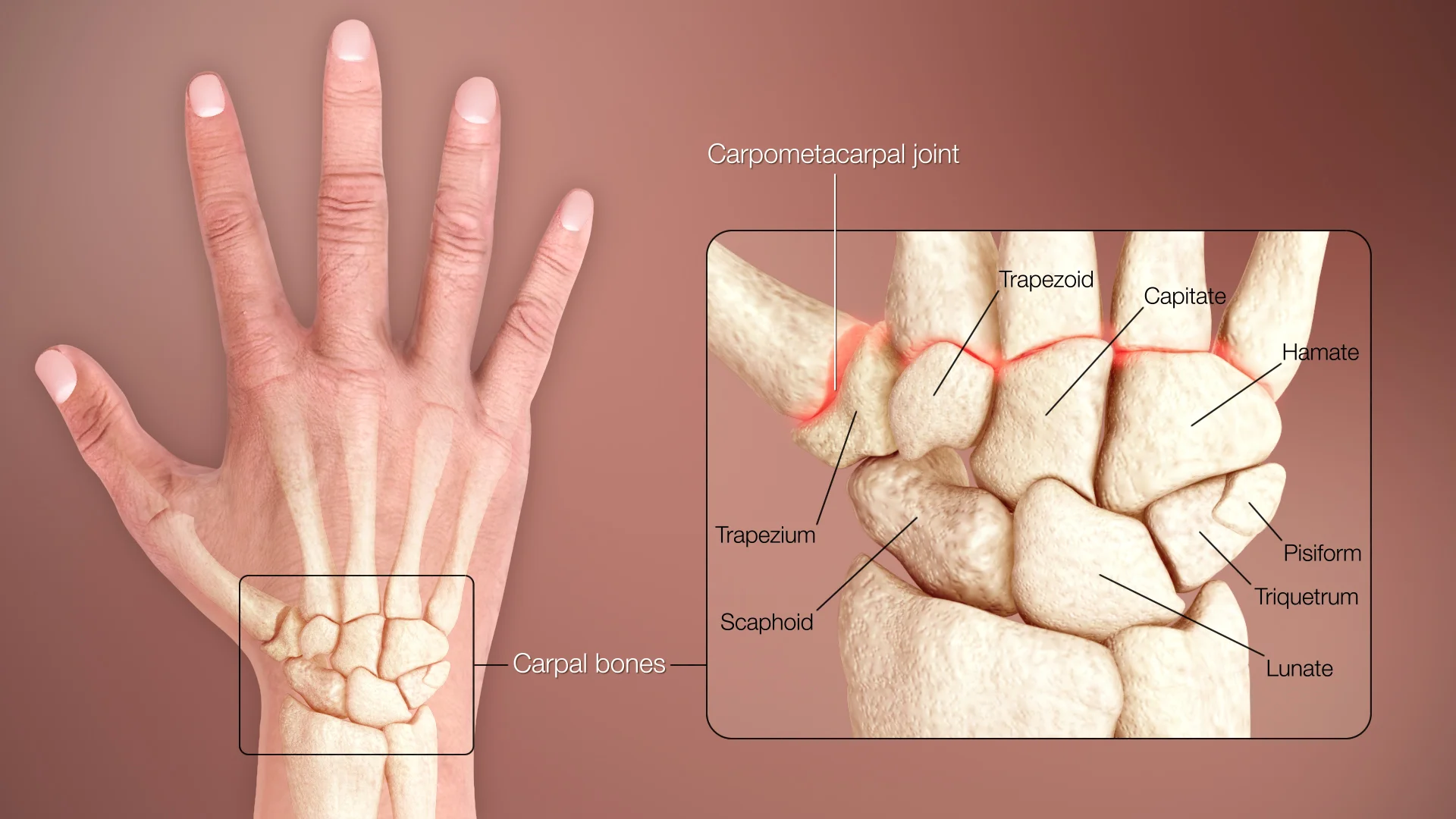
Various bones and joints form this group. The bones that connect make up the wrist are the five metacarpal bones, the carpal bones, and the distal parts of the radius and ulna. The wrist joint is often referred to as the radiocarpal joint.
It is a condyloid synovial joint of the distal upper extremities, moving from the forearm to the hand. Condyloid joints are the portion of ball and socket joints that allow flexion, extension, abduction, and adduction of motion.
Three main joints create the wrist joint. When coupled with a solitary joint, this offers increased stability to the wrist. Your hands and wrists can shift in a wider range of positions and motions as a result, providing you with additional options.
These joints assist the wrist to flex forward, backward, and side to side. They additionally support hand rotation.
Radiocarpal joint: The radiocarpal joint connects the baseline of the wrist bone (the scaphoid, lunate, and triquetrum bones) with its radius, a thicker forearm bone. The thumb side of the wrist is how this joint generally occurs.
Ulnocarpal joint: This joint consists of the lunate, triquetrum, and ulna, the short forearm bone. This joint grows on the side of the wrist’s little finger.
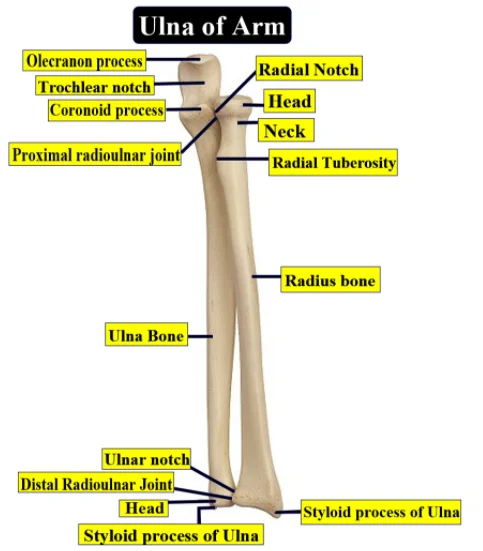
Distal radioulnar joint: Though it develops in the wrist, the wrist bones are not affected. It becomes the ulna and radius at the lower ends.
Structure
The main point of articulation between the carpal bones and the radius lies close to the radius’s distal end.
. At the distal end of the radius, the ulna bone makes a small articulation with the triangular fibrocartilage complex (TFCC), that contributes to the joint further. The scaphoid, lunate pisiform, and triquetrum bones form up the proximal row of the carpal bones, and the trapezium, trapezoid, capitate, and hamate bones bring up the distal row.
The joint capsule is divided into two layers around the wrist joint. In all synovial joints, it is very common. Connections to the carpal, ulna, and radius bones occur by the fibrous outer layer. The inner layer creates a synovial membrane, which produces synovial fluid and lubricates the joint.
Mobility and Stability
The wrist joint enables the hand to move quite freely, which facilitates complicated motions. This puts the wrist joint at risk of damage.
To maintain the wrist joint somewhat stable, internal and external ligaments give support. The small ligaments located between the carpal bones are called intrinsic carpal ligaments, and although they are short and stable, their small size makes them exposed to damage from excessive force or twisting.
Stronger extrinsic ligaments relate the carpal bones of the wrist to the radius and ulna. These connective tissues include the radial and ulnar collateral ligaments but also the palmar/dorsal radiocarpal ligaments.
Blood supply
The radial, ulnar, and interosseous arteries deliver blood to the wrist joint.
The primary blood supply to the wrist joint comes from the radial artery. The anatomical snuffbox is an increase on the lateral part of the wrist, where it enters the wrist. After that, the radial artery branches into many branches, supplying the wrist joint and other tissues.
The blood vessel that gives the wrist joint with blood is the ulnar artery. Where the hamate bone hook connects the pisiform bone at the wrist, a tube referred to as Guyon’s canal forms. The ulnar artery delivers the wrist joint and surrounding regions through some branches.
Small blood vessels found between the radius and ulna bones are known as interosseous arteries. They supply the wrist joint with a different blood supply.
Maintaining the wrist joint’s health and function involves the blood supply to it.
Blood supply issues or injuries may slow healing and raise the risk of effects.
Innervation
The wrist gets innervation from a variety of nerve branches:
- The anterior interosseous branch is the medial nerve.
- The radial nerve’s posterior interosseous branch.
- Dorsal and deep branches start at the ulnar nerve.
Movements of the wrist joint
The wrist has an ellipsoidal (condyloid) synovial joint, importance it can move in two different directions.
This shows flexion, extension, adduction, and abduction can all be performed with the wrist joint.
The forearm muscles are part of every wrist movement.
Flexion
The wrist should be bent to perform a palm motion.
The flexors carpi radialis and ulnaris, with aid from the flexor digitalis superficialis, were mainly responsible for their formation.
Extension
That involves flexing the wrist backward and away from the palm on the hand.
Formed generally by the extensor carpi ulnaris, extensor radialis longus and brevis, and extensor digitorum.
Adduction
For the purpose to do this movement, the wrist must be moved toward the little finger side and the body’s midline.
Formed by the flexor and extensor carpi ulnaris.
Abduction
The wrist moves in such motion from the body’s midline to the side of the thumb.
Flexor carpi radialis, extensor carpi radialis longus, abductor pollicis longus, and extensor carpi radialis brevis produce action.
Pronation
The palm moves downward by rotating the wrist and forearm.
The pronator muscles, which occur on the front side of the forearm, are the principal that control it.
The wrist and forearm move inward toward the body as a result of the relaxation of the pronator muscles.
Supination
The wrist and forearm are rotated in a direction to face the palm straight.
The supinator muscles, which are situated on the posterior side of the forearm, are principally part of maintaining it.
The wrist and forearm rotate outward and away from the body as the effect of the supinator muscles relax.
Circumduction
Using all of the past movements, this movement requires rotating the wrist joint.
A combination of all the muscles used for the other movements regulates it.
The wrist joint’s circular motion gives an optimal range of mobility and flexibility.
Ligaments
Radial collateral ligament: This ligament attaches the scaphoid and trapezium bones to the radius’s styloid process. The lateral side of the wrist joint gets supported by it.
Ulnar collateral ligament: This ligament attaches the triquetrum and pisiform bones to the styloid process of the ulna.
Dorsal radiocarpal ligament: On the dorsal (rear) side of the wrist joint, this ligament goes from the radius to the scaphoid, lunate, and triquetrum bones. It affects how far the wrist can extend.
Palmar radiocarpal ligament: On the palmar (front) side of the wrist joint, this ligament goes from the radius to the scaphoid, lunate, triquetrum, and capitate bones. It restricts the wrist’s flexion.
On the medial side of the wrist joint, the ulna and carpal bones are connected by a group of ligaments and cartilage called the triangular fibrocartilage complex (TFCC). It stabilizes the joint while helping to move weight between the ulna and carpal bones.
Carpometacarpal ligaments: These ligaments support the base of the hand by connecting the carpal and metacarpal bones of the hand.
Ulnolunate Ligament: It connects the ulnocapitate Ligament at the base of the ulnar styloid process after going radially in that motion. Its insertion place is on the ulnar part of the lunate, distal to the short radiolunate ligament.
The ligamentum ulnocapitate: The proximal and volar portions of the capitate are distally attached to the insertion of this ligament. It is proximally shown on the ulnar head’s fovea.
Together, these ligaments allow a wide range of movements while stabilizing the wrist joint.
Muscle attachment
The flexor carpi radialis is a muscle attached at the base of the second and third metacarpal bones. It begins from the medial side of the humeral epicondyle. It allows the wrist joint to flex and abduct.
Given the base of the fifth metacarpal bone and the pisiform bone, the flexor carpi ulnaris muscle is situated in the olecranon process of the ulna and the medial epicondyle of the humerus. It allows the wrist joint to flex and adduct.
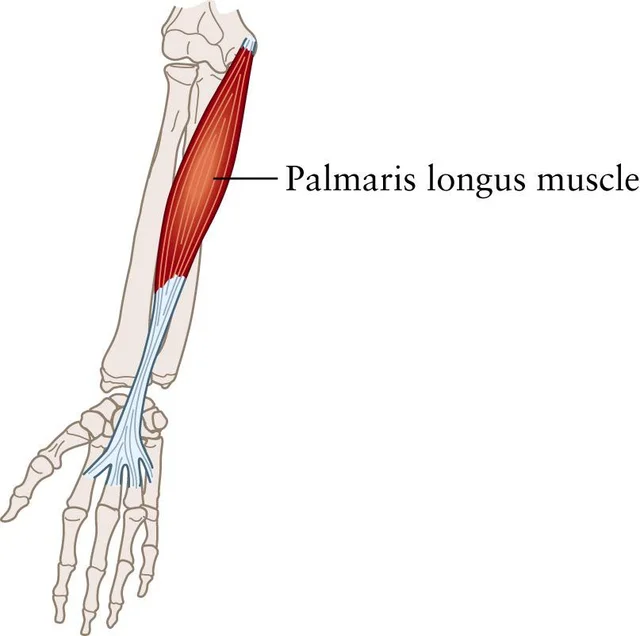
The palmaris longus muscle, which develops from the medial side of the humeral epicondyle, connects to the palmar aponeurosis. Wrist flexion is established.
The extensor carpi radialis longus muscle actually connects to the base of the second metacarpal bone with the lateral epicondyle of the humerus. This muscle is for the wrist joint’s abduction and extension.
The base of the third metacarpal bone is formed by the extensor carpi radialis brevis muscle, which develops on the lateral side of the humerus epicondyle. It maintains the wrist joint’s flexion and extension.
Extensor carpi ulnaris: This muscle connects to the base of the fifth metacarpal bone and arises from the lateral side of the humerus epicondyle and the posterior borders of the ulna. The wrist joint’s adduction and extension happen by these muscles.
The flexor digitorum superficialis is a muscle that attaches to the middle phalanges of the four fingers and starts from the radius, the coronoid process of the ulna, and the medial epicondyle of the humerus.The two fingers and the wrist joint flex.
The flexor digitorum profundus muscle connects to the distal phalanges of the four fingers after starting from the ulna and the interosseous membrane. Every finger and wrist joint flex.
Extensor digitorum: This muscle connects to the extensor expansion of the four fingers and starts from the posterior border of the ulna and the lateral epicondyle of the humerus. It extends the fingers and wrist joint.
Together, these muscles allow the wrist joint to move in a variety of methods, including flexion, extension, abduction, and adduction.
Tendons
Strong, connective tissue called tendons assist muscles in following bones. Many tendons connect the hand bones to the forearm muscles at the wrist joint, allowing movement of the fingers and wrist.
The following tendons move through the wrist joint:
- Flexor tendons: This muscle attaches to the base of the second and third metacarpal bones, and also to the medial aspect of the humeral epicondyle. It flexes and takes the wrist joint.
- Extensor tendons: These tendons arise from the forearm muscles and connect with the finger bones. Their role is to straighten the wrists and fingers.
- The tendons located on the sides of the wrist, called the ulnar and radial deviation tendons, are what enable the wrist to move from side to side.
- Thumb tendons: The flexor, extensor, and abductor pollicis longus are three of the tendons that manage thumb movement.
A decreased range of motion, pain, and edema may arise from disorders or injuries that affect the tendons in the wrist joint. Tendonitis, an inflammation of the tendons, tenosynovitis, which is inflammation of the tendon sheath, and carpal tunnel syndrome, which is compression of the median nerve as it goes through the wrist, are common problems. Rehabilitation treatments involve physical therapy, rest, and in more serious cases, surgery.
Clinical significance
The median nerve, which goes through the wrist’s carpal tunnel, has been compressed, and results in this disorder.
It may occur from repetitive activities like typing or using a computer mouse, as well as diseases like pregnancy or arthritis that enlarge the wrist.
Carpal tunnel syndrome is defined by hand and finger pain, tingling, and numbness, especially at night.
A wrist splint, anti-inflammatory drugs, or surgery for decreasing pressure on the nerve are possible ways of treatment.
Wrist sprains and strains
The root of these injuries is a fracture or stretching of the wrist muscles or ligaments. These may occur from overuse from repeated movements or from sudden impacts like falls or sports injuries.
Pain, swelling, and a decreased range of motion for carpal tunnel syndrome are symptoms of a sprain or strain of the wrist.
Surgery in critical situations is one possible method of treatment, with physical therapy and rest, ice, compression, and elevation (RICE).
Tendinitis
The condition arises when the wrist tendons become irritated or inflamed. It can be brought on by disorders that cause wrist swelling or by repetitive activities like typing or playing sports. Tendinitis symptoms involve wrist pain, swelling, and problems moving the wrist. Some possible therapies involve physical therapy, medication for inflammation, and RICE (rest, ice, compression, and elevation).
Arthritis
Joint inflammation and stiffness are symptoms of a medical disorder called arthritis. It may affect the wrist joint, causing discomfort, edema, and decreased movement. Wrist arthritic symptoms include pain, stiffness, and swelling. Physical therapy, surgery, or specific drugs to reduce inflammation may all be involved in the treatment.
Ganglion cysts
These tendons or wrist joint nodules are not cancers. These could result from repetitive actions or injuries to the wrist. A visible bulge on the wrist, pain, and a restricted range of motion are symptoms of a ganglion cyst. In severe cases, options for treatment may include surgery, aspiration (by removing fluid from the cyst), and RICE (rest, ice, compression, and elevation).
De Quervain’s tenosynovitis
The disease arises from inflammation or irritation of the tendons that control thumb mobility. Conditions leading to wrist swelling can have a cause, as well as repeated movements such as gripping or twisting. Pain and swelling at the base of the thumb and wrist are symptoms of De Quervain’s tenosynovitis. Physical therapy, anti-inflammatory medications, and rest, ice, compression, and elevation (RICE) are various types of treatment. Major conditions might require surgery.
FAQs
What is the joint of the wrist?
The wrist joint, which is found between the hand and forearm bones, assists the movement of the wrist and hands.
What may cause wrist joint pain and restrict the wrist’s range of motion?
Pain, swelling, and decreased range of motion can be caused on by disorders or injuries that affect the tendons in the wrist joint.
How is difficulty in the wrist joint treated?
Treatment options for joint pain in the wrists can involve physical therapy, rest, or surgery, depending on the intensity and underlying basis for the pain.
Is there a way to avoid wrist joint pain?
Having sufficient technique during physical activity, taking breaks to relax and stretch the wrist, and maintaining proper posture are all methods to decrease wrist joint pain.
References
- Patel, D. (2023, June 10). You searched for a wrist joint – Mobile Physiotherapy Clinic. Mobile Physiotherapy Clinic. https://mobilephysiotherapyclinic.in/?s=wrist+joint.
- Dhameliya, N. (2022, April 22). WRIST JOINT. Samarpan Physiotherapy Clinic. https://samarpanphysioclinic.com/wrist-joint/


10 Comments