Shoulder Dystocia
Shoulder Dystocia: What is it?
When one or both of your baby’s shoulders become trapped inside your pelvis during childbirth, it’s known as shoulder dystocia. The Greek words “dys,” which means difficult, and “tokos,” which means birth, are the roots of dystocia.
Shoulder dystocia is a medical emergency. Usually, babies born with this syndrome are safe. However, it can lead to significant issues for both you and your child.
What is the Prevalence of Shoulder Dystocia?
The disorder known as shoulder dystocia is uncommon. Because the illness is occasionally overdiagnosed or underdiagnosed, statistics vary greatly. The baby’s birth weight also affects the average rate. 0.6% to 1.4% of newborns weighing between 5 pounds, 8 ounces, and 8 pounds, 13 ounces have shoulder dystocia. The percentage of newborns weighing more than 8 pounds, and 13 ounces rises from 5% to 9%.
Causes of Shoulder Dystocia:
Shoulder dystocia may not always be predictable. Shoulder dystocia during vaginal birth is more likely to develop, nevertheless, due to certain variables. These consist of:
- You have diabetes.
- You were diagnosed with gestational diabetes.
- You’re far too fat.
- You have a narrow pelvic opening or a modest height.
- On prenatal ultrasounds, your baby seems huge.
- You previously gave birth and suffered from shoulder dystocia.
Which Symptoms indicate Shoulder Dystocia?
Although there are risk factors for shoulder dystocia, anybody can develop the disorder. The occurrence of shoulder dystocia cannot be predicted, and there are no symptoms. It’s possible that your obstetrician won’t become aware of the issue until after you give birth.
When your baby’s head emerges and then pulls back in against the perineum—the space between your vagina and rectum—it becomes evident. For this, we call it the “turtle sign.”
How is Shoulder Dystocia Diagnosed?
Three criteria must be satisfied for your obstetrician to diagnose shoulder dystocia:
- You have successfully delivered your baby’s head, but you are unable to push out their shoulders.
- The head of your kid has been out for at least a minute, but the body has not yet out.
- For your baby to be delivered safely, medical intervention is required.
What is the Treatment for Shoulder Dystocia?
If you have diabetes or your baby is unusually large, your obstetrician could suggest that you schedule a C-section.
Your healthcare professional will have a safety checklist prepared if you are at risk for shoulder dystocia and are giving birth vaginally. The steps to follow in the event of shoulder dystocia are outlined in a safety checklist.
If your obstetrician determines that you have shoulder dystocia, the birth process will go quickly. The nursing staff and your obstetrician may attempt several techniques. To broaden your pelvis, they might want to reposition you into a better posture. Alternatively, they might wish to shift your baby’s shoulders into a better fetal position.
The HELPERR mnemonic is a strategy your healthcare team may use to address shoulder dystocia. HELPERR stands for:
H— Help: Your obstetrician will make a call for assistance. They will make use of the safety checklist and request further assistance from other medical professionals. These providers might include additional labor and delivery, a neonatologist, and an anesthesiologist. The equipment you need will be delivered to your room.
E — Assess for episiotomy: Your obstetrician will determine if you must have an episiotomy to help birth your baby. A cut (incision) made in the perineum to enlarge the vaginal entrance is called an episiotomy. Only if they need to create space for rotation maneuvers will your provider carry out this technique.
L — Legs: Your obstetrician may employ the McRoberts technique. With the McRoberts technique, your obstetrician will instruct you to squeeze your thighs up against your tummy (abdomen). This technique aids in pelvic rotation and flattening.
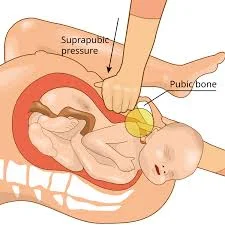
P—Pressure: Your obstetrician might apply pressure above the pubic region. Your obstetrician will use suprapubic pressure, which is pressure applied to the abdomen above the pubic bone. It tries to twist and deliver your baby by applying pressure on its shoulder.
E – entrance maneuvers: Internal rotation or entrance maneuvers may be performed by your obstetrician. In an attempt to turn your baby, an obstetrician will reach up into your vagina.
R — Remove the posterior arm: The Jacquemier’s procedure may be used by your obstetrician. Your doctor will remove one of your baby’s arms from the delivery canal using the Jacquemier maneuver. Their shoulders could pass through more easily as a result.
R— Roll the patient: The Gaskin maneuver may be used by your obstetrician. Your obstetrician will advise you to roll onto your hands and knees to do the Gaskin manoeuvre, which involves changing positions.
Your obstetrician may choose one of the following strategies in extreme situations when no other approaches are effective:
- Clavicle fracture: To free your baby’s shoulders, your obstetrician will break their collarbone.
- Zavanelli maneuver: Your obstetrician will force your baby’s head back into your uterus and conduct a C-section.
- Symphysiotomy: To widen your pelvic opening, an obstetrician will create an incision in the cartilage between your pubic bones.
Delivery Methods For Shoulder Dystocia:
Mild shoulder dystocia: The doctor and a helper put moderate pressure on the baby’s midline with their hand right above the mother’s pubic bone. This helps to shift the back shoulder down, dislodging it from the pelvic bone.
At the same time, the McRoberts Manoeuvre is completed. It takes the assistance of two people to withdraw your legs from the stirrups and flex them back against your abdomen. This repositions your pelvic bones, allowing the baby more room to be birthed.
Moderate dystocia in the shoulders. If it doesn’t work, your doctor could do a posterior arm delivery, in which the baby’s arm is detected and stretched out of the vagina towards the rear of the mother. By doing this, the shoulder dystocia impaction may be lessened, allowing for the delivery of the infant.
One strategy your doctor might try is the Woods’ Screw Manoeuvre. Your doctor applies pressure on your baby’s front shoulder while rotating them in a twisting motion. The doctor uses the Rubin Manoeuvre to gently move your baby from side to side by applying external pressure to your belly. To help with this technique, the doctor may gently press on your baby through the vaginal canal.?
The physician may even decide to do an episiotomy throughout all of these efforts. This is an incision made along your perineum to provide room for the delivery of your baby.?
Severe dystocia in the shoulders. It is possible to break the baby’s collarbone to facilitate passage. Your doctor could push and rotate your baby’s head back into your vagina using a cephalic replacement if this doesn’t work.
To reduce the amount of oxygen your baby loses, this promotes blood flow down the umbilical cord, allowing for a C-section.
What are the Possible Complications of Shoulder Dystocia?
Shoulder dystocia during labor can cause complications for both you and your unborn child.
Issues that might impact you:
- Severe, prolonged bleeding following childbirth (postpartum hemorrhage).
- Severe tearing of the perineum, the region between the vagina and the anus.
- An irregular connection between your vagina and rectum is known as a rectovaginal fistula.
- A uterine rupture occurs when your uterus rips during childbirth.
- Release your pubic bones.
Complications that may impact your baby
When your infant has shoulder dystocia, brachial plexus palsy is the most prevalent consequence. The brachial plexus nerves travel through your baby’s arm from the spinal cord in the neck. These nerves are in charge of giving your baby’s hand, arm, and shoulder sensation and movement. Weakness and paralysis on the affected side may result from damage to these nerves.
Additional issues for your child might be:
- Fractures to your baby’s humerus (upper arm bone) or clavicle (collar bone).
- An uncommon condition that affects your baby’s face and eyes is called Horner’s syndrome.
- Compressed umbilical cord: This occurs when the cord becomes stuck between your pelvic bone and your baby’s arm. A flattened umbilical cord might prevent your baby from receiving oxygen and blood. Although extremely uncommon, this can result in death or brain damage.
What are the Risk factors for Developing Shoulder Dystocia?
Shoulder dystocia is a common condition. The disease primarily affects infants with normal birth weights. However, several risk factors make the illness more likely. Among these risk factors are:
Diabetes: Both gestational diabetes and pre-existing diabetes might result in a big baby. Individuals with diabetes are 20% more likely to give birth to a child that weighs more than 8 pounds, 13 ounces.
Macrosomia: If your baby weighs more than 8 pounds, 13 ounces at delivery, they are said to have macrosomia. Your healthcare professional can suggest a C-section if your baby is large.
- A history of shoulder dystocia during pregnancy.
- Having twins or other multiples during pregnancy.
- Being overweight or gaining too much weight when pregnant.
- Little in stature.
- Abnormality of the pelvis.
- Over 35 years old.
- Delivering a baby past your due date.
Additionally, several labor and delivery-related disorders may increase the chance of shoulder dystocia. Among these risk factors, assisted vaginal birth is the most prevalent. To assist in delivering your baby via the birth canal, your obstetrician will need to utilize either forceps or a vacuum extractor. During labor and delivery, additional risk factors might include:
- Using oxytocin as a labor inducer.
- Administering an epidural.
- Extremely protracted contraction period, the first stage of labor.
- The extremely brief or lengthy pushing phase is the second stage of labor.
- Delivering your baby with improper pressure or techniques.
How can Shoulder Dystocia be avoided?
Shoulder dystocia is a common condition. The majority of occurrences are unavoidable and occur in infants with normal birth weights.
- Control your diabetes.
- Keep your weight in check during your pregnancy.
- Enquire with your doctor about bringing on labor.
- Give your healthcare practitioner a call if your due date has passed.
- Talk to your physician about the potential of a C-section.
- Think about skipping labor drugs like an epidural.
What’s the Prognosis for Shoulder Dystocia?
According to research, half of all newborns with shoulder dystocia are fully functional by the time they are three months old. Eighty-two percent of newborns are fully functional by the time they are 18 months old.
The results of your child’s brachial plexus damage are usually favorable. However, certain actions could have an impact on your child’s long-term results. They could struggle to utilize their damaged limb for other purposes and with fine motor skills. Within six to twelve months, almost 90% of these injuries go away. Permanent damage occurs in less than 10% of cases.
Your risk of developing shoulder dystocia again is increased by 15% if you have had a baby with the disorder. If you intend to have more children, make sure to talk about this with your healthcare professional. The vaginal birth after a cesarean (VBAC) procedure is not advised if you had a C-section because of shoulder dystocia.
FAQs
Why does shoulder dystocia occur?
The constant anterior-posterior posture of the fetal shoulders as they concurrently descend or enter the pelvic inlet is the fundamental cause of shoulder dystocia.
How should one handle shoulder dystocia?
Good delivery is nearly always achieved by using release techniques such the knee to chest (McRoberts manoeuvre), suprapubic pressure, posterior arm or shoulder delivery, and internal rotational manoeuvres with composure and consideration.
What are the long-term consequences of shoulder dystocia?
Both the mother and the child may experience long-term issues as a result of shoulder dystocia. Depending on how serious the damage is, they can take many different forms. While some newborns may be permanently disabled, others may not have any long-term issues at all.
Does dystocia in the shoulders go away?
This is usually just temporary, and movement will return within a few hours or days. For every 100 babies with shoulder dystocia, one will have permanent damage. Shoulder dystocia can also lead to additional issues, such as fractures of the infant’s arm or shoulder. These often heal without any issues.
How can shoulder dystocia be recognized?
You are unable to push your baby’s shoulders out after delivering their head.
Your baby’s head has been out for at least a minute, but their body hasn’t followed.
For your baby to be delivered safely, medical assistance is required.
How is dystocia treated?
Dystocia can be treated surgically with a cesarean section or medically with uterotonic (or ecbolic) drugs and aided fetal evacuation.
Which posture is ideal for preventing shoulder dystocia?
The rate of infant injury is decreased when shoulder dystocia is treated using the hands-and-knee posture as the initial treatment. No issues were noticed throughout the procedure. It should be included in clinical practice for a safer birth.
What are some ways to avoid dystocia?
Shoulder dystocia is usually unpredictable and hence cannot be prevented. If you have diabetes or develop it during pregnancy, you will often be given a scheduled cesarean section or an early induction of labor. Shoulder dystocia risk will be decreased as a result.
References
- Shoulder dystocia. (2025, March 19). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/22311-shoulder-dystocia
- What is shoulder dystocia? (2023, May 27). WebMD. https://www.webmd.com/baby/what-is-shoulder-dystocia
- Dystocia. (2022, March 10). https://patient.info/doctor/dystocia